Section 4 Provider Survey
4.1 Current Landscape
This section describes the current landscape of early childhood data collection at participating child care and pre-k sites and nonprofit, government, and healthcare organizations serving young children. It includes information on what data is currently being collected, who is collecting that data, current use of electronic databases, current data collection requirements for organizations serving children, how data is being shared, and how data is currently being used.
4.1.1 Data Being Collected
This section describes data currently being collected by participating child care sites and pre-k and nonprofit, government, and healthcare organizations serving young children. It describes the percentage of these sites that are currently collecting data on children and families, developmental and other assessments, and screenings; how that data is currently being collected and stored; whether or not child care sites and nonprofit and government organizations would be willing to collect data that they are not currently collecting and entering it into an electronic database; and whether or not they would need additional resources to do so.
4.1.1.1 Data on Children and Families
This section describes the data on individual children and families that are currently being collected by participating child care and pre-k sites and nonprofit, government, and healthcare organizations serving young children. It describes the percentage of these sites that are currently collecting this data; how this data is currently being collected and stored; whether or not child care sites and nonprofit and government organizations would be willing to collect data that they are not currently collecting; and whether or not they would need additional resources to do so.
4.1.1.1.1 Child Care Providers
Figure 4.1: Information child care providers collect on children and how it is stored
Figure 4.1 shows that child care provider sites participating in the survey generally reported that the demographic information listed on the x-axis of the graph are collected and that the data is frequently stored in some sort of electronic database. Notably, whether or not the child was receiving WIC was less commonly collected and entered into some sort of electronic database. Whether or not a child was receiving WIC, participating in Medicaid, or experiencing homelessness were the categories of demographic information that respondents most often identified as information that they would not or could not collect on children even with additional resources, but some provider sites did indicate a willingness to gather this information.
Figure 4.2: Information child care providers collect on families and how it is stored
Compared to Figure 4.1, Figure 4.2 shows that information on families is less commonly and consistently gathered and stored by provider sites participating in the survey. Information on caregivers’ educational attainment and income or income range were the pieces of information most commonly entered as fields in electronic databases, and educational attainment, enrollment in school or job training, and referrals to other organizations for services were the kinds of information most commonly collected but noted on paper documents or a notation field in a database. Notably, about 13-34% of provider sites participating in the survey reported that they would not collect the information listed on parents, even with additional resources. And, 14-38% of provider sites participating in the survey reported that they would only collect this information with additional resources.
4.1.1.1.2 Other Nonprofits and Government Agencies
Results suggest that a majority of respondents are collecting basic demographic information of the children and families they serve. Some of the more specific information such as child care subsidy and WIC status are collected less frequently or not at all. In conversations with respondents some reported that data captured by providers is only the information that is relevant to the program. Additionally, sometimes the collection and storage of certain data elements are dependent on the context and whether certain information is collected elsewhere. For example, one respondent from a governmental agency reported that their program only collects child care subsidy information if there is no income information available or if they do not know about their SNAP or Medicaid eligibility. There was also some discussion that particular providers may be aware about certain information about a child or family, such as WIC recipient status, but they are not collecting or storing that information.
About 10 respondents reported that they collect additional information such as medical and health behavior information (e.g., smoking status), domestic or intimate partner violence, or SSI/disability status. Results suggest that how certain agencies or programs are storing information are a bit more idiosyncratic. Sometimes there is a dropdown menu for providers to store information systematically and other times there is only a general field or note area in the electronic database. Further, respondents reported that sometimes there is a mix of notes and paper. One provider notes that they use paper charts themselves but that the state has an electronic database that they must use.
4.1.1.2 Assessments
This section describes the developmental and other assessments currently being conducted by participating child care and pre-k sites and nonprofit, government, and healthcare organizations serving young children. It describes the percentage of these sites that are currently collecting this data; how this data is currently being collected and stored; willingness to collect data that they are not currently collecting; and the need for additional resources to do so.
4.1.1.2.1 Child Care Providers
Figure 4.3: Developmental and other assessments child care providers conduct and how they are stored
Figure 4.3 shows that with the exception of Teaching Standards GOLD (TSG), provider sites participating in the survey are generally not conducting the developmental and other assessments listed and entering them into an electronic database. About 35% of sites surveyed indicated that they currently both collect this information and enter it into the fields of an electronic database, and an additional 10% of sites indicated that the assessment was conducted but only stored on paper notes or a notes field. After TSG, participating sites reported using the Developmental Assessment of Young Children (DAYC) and Developmental Indicators for Assessments of Learning (DIALs) assessments the most frequently. About 31% and 29% of participating sites, respectively, reported using these assessments. However, only 11% of participating sites reported currently entering the DIALs assessment into the fields of an electronic database, and about 9% of sites reported entering DAYC results into an electronic database. TSG, DAYC, and DIALS were also the three assessments that the smallest number of sites reported that they would not conduct even with additional resources, with about 23-33% of sites reporting that they would not conduct it.
When offered the option to report additional assessments that they conducted, some participating sites reported using the Ages and Stages Parent Questionnaire, Early Learning Accomplishment Profile (E-LAP), and Learning Accomplishment Profile (LAP-3). Some providers also reported conducting company-specific assessments and not being familiar with the assessments included in the survey.
4.1.1.2.2 Other Nonprofits and Government Agencies
A majority of respondents indicated that they are not conducting developmental assessments. Further, more respondents reported that they would not collect the information with additional resources than those who reported they would with or without additional resources.
Qualitative responses show that some providers are perhaps asking questions from a development assessment instrument or are at least related to the assessment topic, but they are not using a standardized tool. Additionally, some providers rely on other agencies or organizations to administer development assessments. One provider noted that they would like to see complete information from the assessments/screeners for a more holistic view of the child, but is aware of certain privacy restrictions.
4.1.1.3 Screenings
This section describes the developmental and other assessments currently being conducted by participating child care and pre-k sites and nonprofit, government, and healthcare organizations serving young children. It describes the percentage of these sites that are currently collecting this data; how this data is currently being collected and stored; willingness to collect data that they are not currently collecting; and the need for additional resources to do so.
4.1.1.3.1 Child Care Providers
Figure 4.4: Screenings child care providers conduct and how they are stored
Figure 4.4 shows that the majority of participating child care provider sites are not currently conducting the screenings listed on the x axis of the graph, but between 15% and 26% of all participating providers reported being willing to conduct the screenings listed with additional resources. Notably, 21% to 64% of providers reported that they would not conduct the screenings listed even with additional resources. In addition, only 21-24% percentages of participating sites reported that they would not conduct the two Ages and States Questionnaires, dental screenings, and vision screenings. About a third of participating sites reported that they would not conduct autism screenings, and about half reported that they would not conduct the other screenings listed. Among the sites that reported currently conducting some of the screenings, the most commonly conducted screenings were the two Ages and Stages Questionnaires, which were entered into electronic databases at about a third of the sites participating, and vision and dental screenings, which were only entered into electronic databases at about 10% of participating sites.
In open-ended fields, one respondent reported that they collect and use the information stored in children’s files, but that the information is kept under lock and key and only used by need to know personnel.
4.1.1.3.2 Other Nonprofits and Government Agencies
The most common screenings providers reported utilizing were the Edinburgh Postnatal Depression Scale (EPDS), the Patient Health Questionnaire (PHQ), Elevated Blood Levels, and Dental with 4 respondents indicating that information is collected. About 56% of respondents noted additional screenings such as an adult adolescent parenting inventory and intimate partner violence are performed at their agency. Further, depending on the program the screenings may be performed multiple times. Sometimes screenings are tied to developmental milestones or are calendared where they need to be performed more than once in a year.
As with the previous section on developmental assessments, qualitative responses show that some providers are perhaps asking questions from a screening instrument or are at least related to the screener topic, but they are not using a standardized tool. Additionally, some screenings (formal and informal) are only performed if the context of the child/family they serve warrants the screening.
4.1.2 Who Collects the Data?
This section describes who currently collects data on individual families and children and conducts screenings and assessments at participating child care and pre-k sites and nonprofit, government, and healthcare organizations serving young children.
4.1.2.1 Data on Children and Families
4.1.2.1.1 Child Care Providers
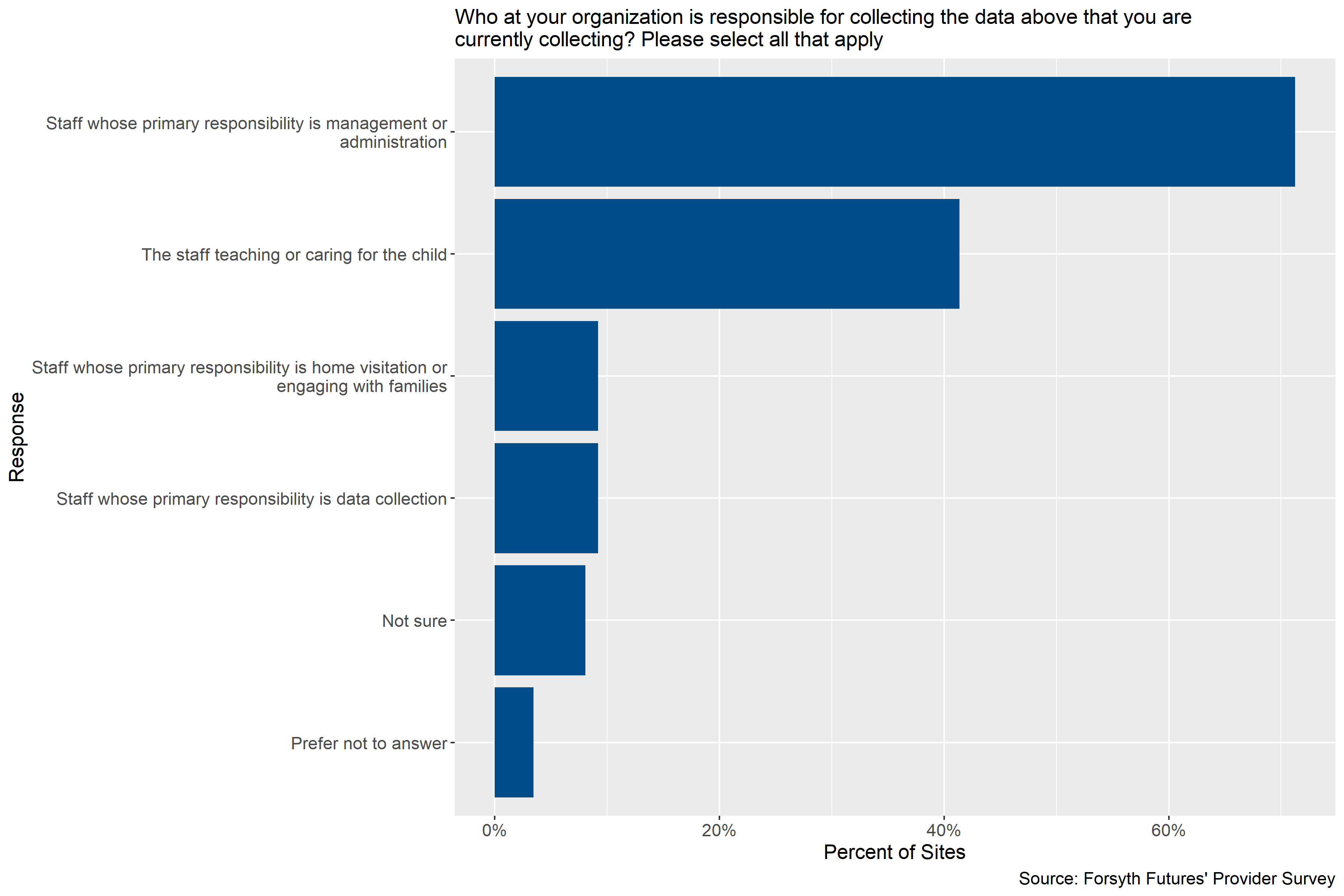
Figure 4.5: Child care provider staff responsible for collecting data on children and families
Figure 4.5 shows that participating child care provider sites reported that the staff responsible for collecting data on families and children was most often staff whose primary responsibility is management or administration (about 71% of sites), followed by the staff teaching or caring for the child (a little more than 40% of sites). However, a small number of sites reported that home visitation staff or staff whose primary responsibility is data collection are responsible for collecting this information. In open-ended fields on the survey, some providers noted that they themselves and / or the owners (and sometimes only staff in the context of child care homes) collected this information. One respondent reported that the parents supply the information, and one respondent reported that they were not collecting the information.
4.1.2.1.2 Other Nonprofits and Government Agencies
The majority of respondents indicated that staff whose primary responsibility is management/administration or home visitation are the ones responsible for collecting background information (e.g., demographics, WIC recipient status) on the people they serve. One respondent did note that they have office support staff that handles their data collection while clinical providers noted that many are involved in collecting data on their patients given the nature of clinical treatment.
4.1.2.2 Assessments and Screenings
4.1.2.2.1 Child Care Providers
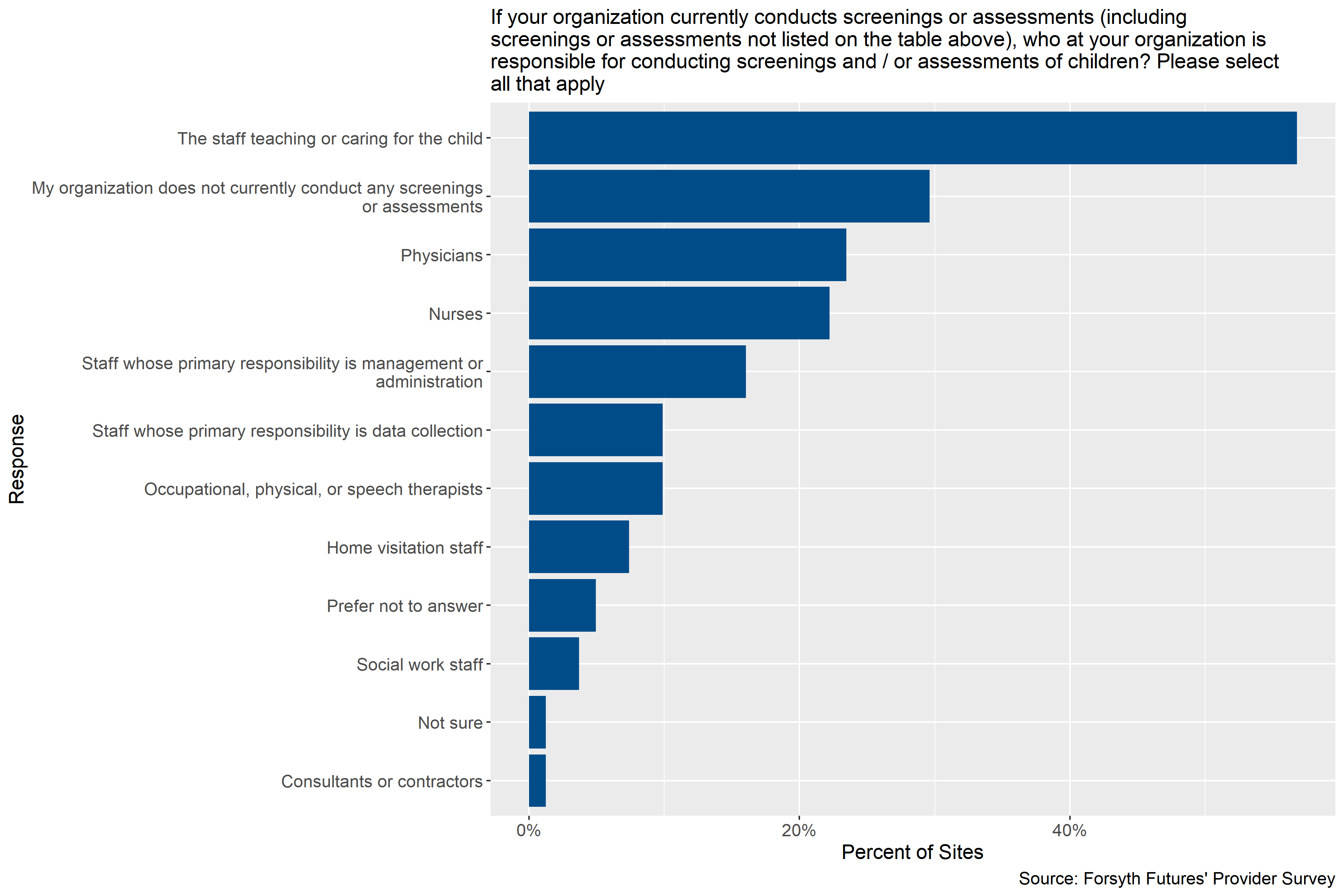
Figure 4.6: Child care provider staff responsible for conducting screenings or assessments
Figure 4.6 shows that participating child care provider sites who conduct screenings or assessments reported that the staff teaching or caring for the child were most often collected by the staff teaching or caring for the child. Physicians and nurses were also commonly reported as the person responsible for conducting screenings or assessments. It is not clear from the survey if these physicians and nurses are on site with providers or if respondents were referring to children’s primary care physicians in answering this question.
In the open-ended fields of the survey one respondent indicated that they have someone come on site to conduct vision and dental screenings on an annual basis and that they partner with a speech therapist that will connect with parents if the provider refers them. One respondent also indicated that they have parents complete the Ages and Stages Questionnaire online.
4.1.2.2.2 Other Nonprofits and Government Agencies
A variety of staff members are responsible for administering assessments/screenings. The most frequent response with 5 each was that staff teaching or caring for the child and home visitation staff are responsible. About 2 respondents reported they do not administer assessments/screenings themselves. Additionally, qualitative responses suggest that many others are involved and they range from clinicians and counselors to nutritionists. Sometimes the person responsible is not consistent and depends on the settings and/or context.
4.1.3 Electronic Databases
This section describes the use of electronic databases by participating child care and pre-k sites and nonprofit, government, and healthcare organizations serving young children. It includes information on the percentage of providers and agencies currently using electronic databases, which electronic databases are being used, and staff currently responsible for entering information into these databases.
4.1.3.0.1 Child Care Providers
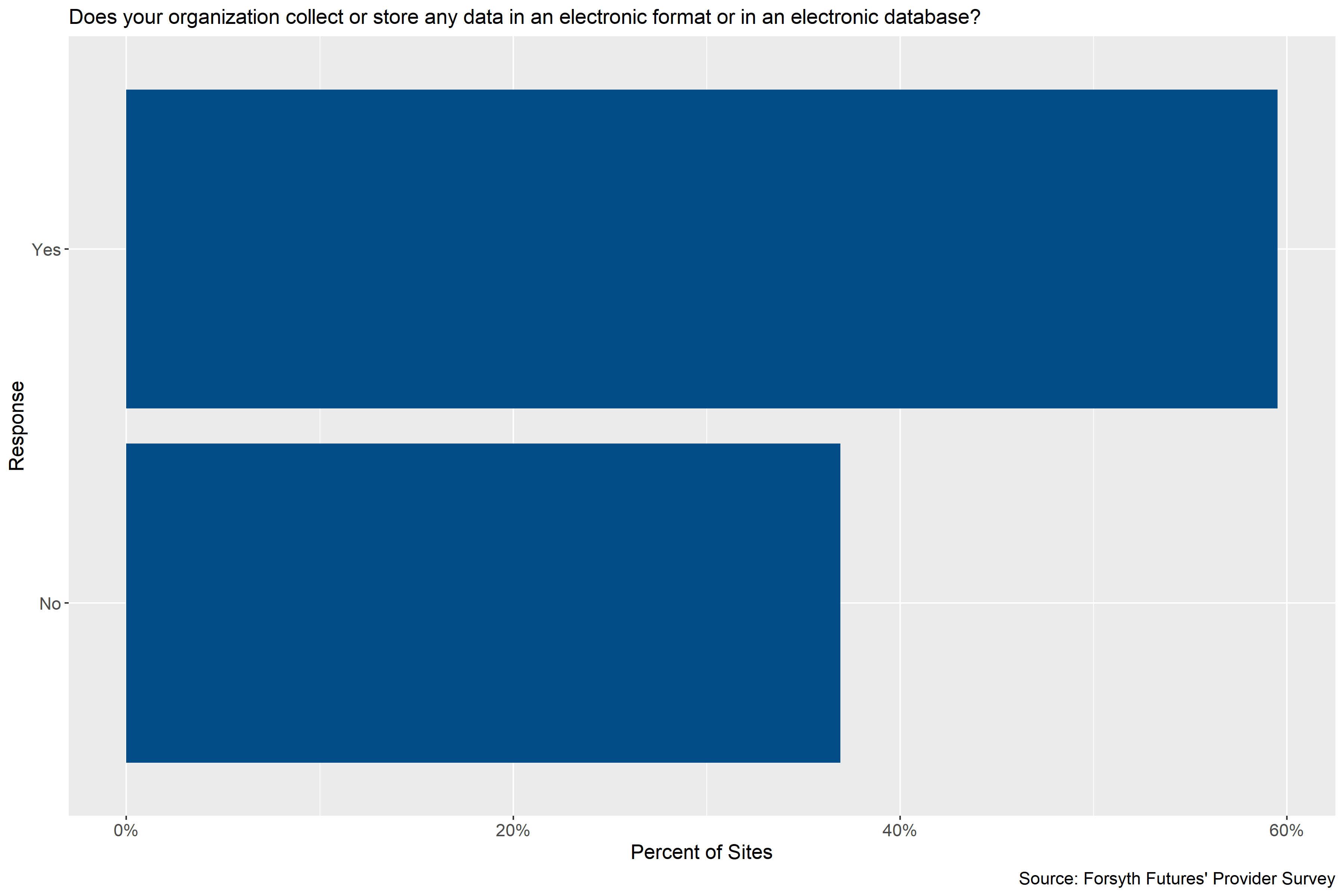
Figure 4.7: Percentage of child care sites using an electronic database
Figure 4.7 shows that the majority of child care provider sites participating in the survey, just under 60%, reported that they collect or store some data in an electronic database.
4.1.3.0.2 Other Nonprofits and Government Agencies
All 16 respondents reported that their program collects or stores at least some data electronically.
4.1.3.1 Electronic Databases Used
4.1.3.1.1 Child Care Providers
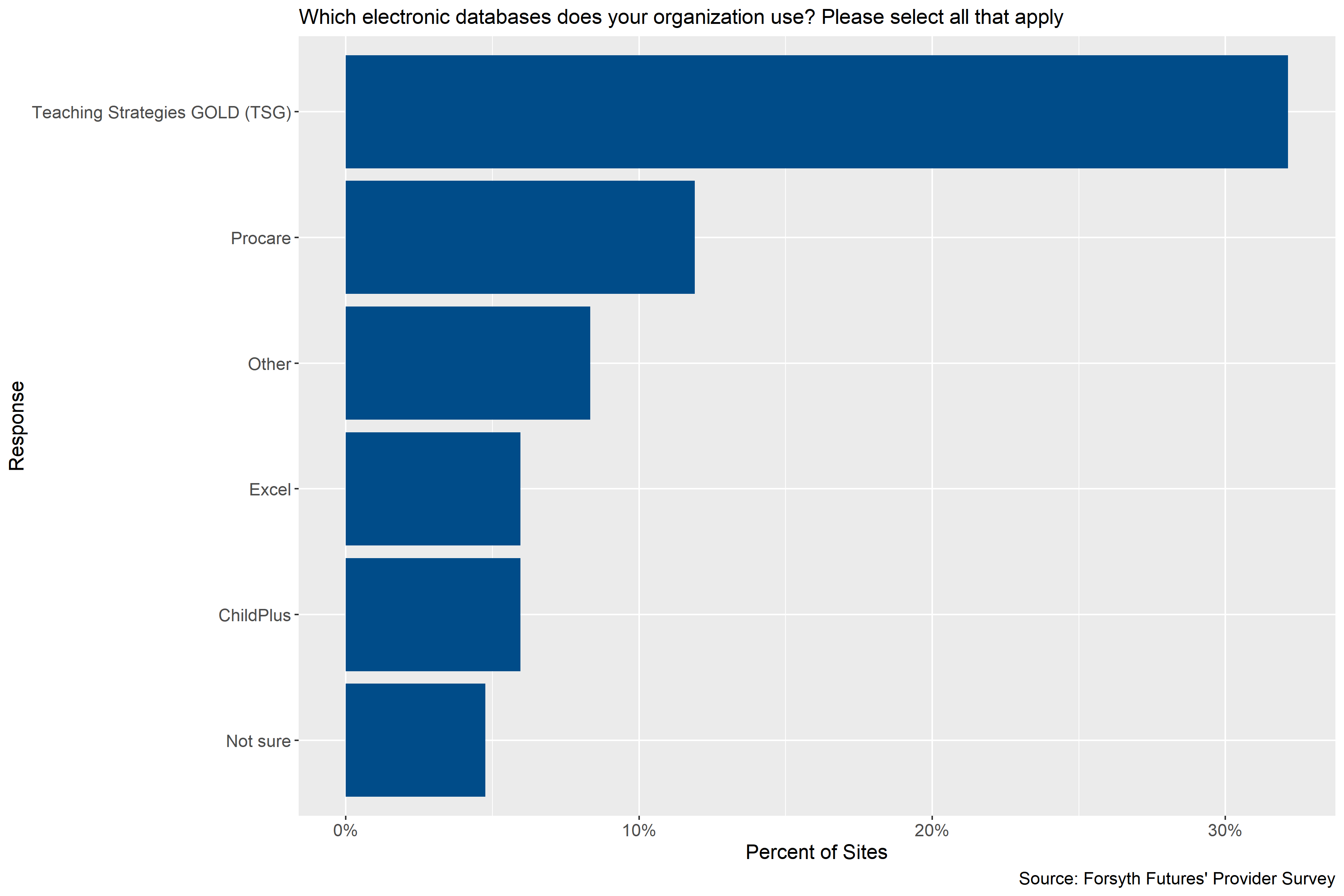
Figure 4.8: Electronic databases used by child care sites (percentage is out of all participating sits
Figure 4.8 shows that Teaching Strategies GOLD (TSG) was the most commonly used electronic database among child care sites participating in the survey, with about a third of sites reporting its use. A smaller percentage of sites reported using Procare, ChildPlus, Excel, or another database not listed. Participating sites that reported using electronic databases other than what was listed on the survey instrument reported using DayCare Works, FACTS, RenWeb, Minute Menu, Office Center Emerging Technologies, and databases specific to their companies.
4.1.3.1.2 Other Nonprofits and Government Agencies
About 55% of the electronic databases listed in the table were selected by respondents. Epic and Excel were the most commonly selected with Apricot, Health Information System, and Visit Tracker as the other selected responses. In conversations with providers, 75% either reported using additional databases or noted that they were transitioning to another software in the near future. Most respondents discussed additional software systems such as WorkLife Systems, Google Docs and Sheets, and Fabric among a few others. Some of the software providers are mandated by the state or program itself. Additionally, a few respondents noted that there are a variety of softwares–mandated or not mandated by the state or program–that their agency uses. For example, one respondent noted that across four of the agency programs each was using a different data management system. Further, some respondents may be using certain systems, such as Epic, to only access information and not necessarily using it for data entry/storage.
4.1.3.2 Staff Responsible for Entering Data in Electronic Databases
4.1.3.2.1 Child Care Providers
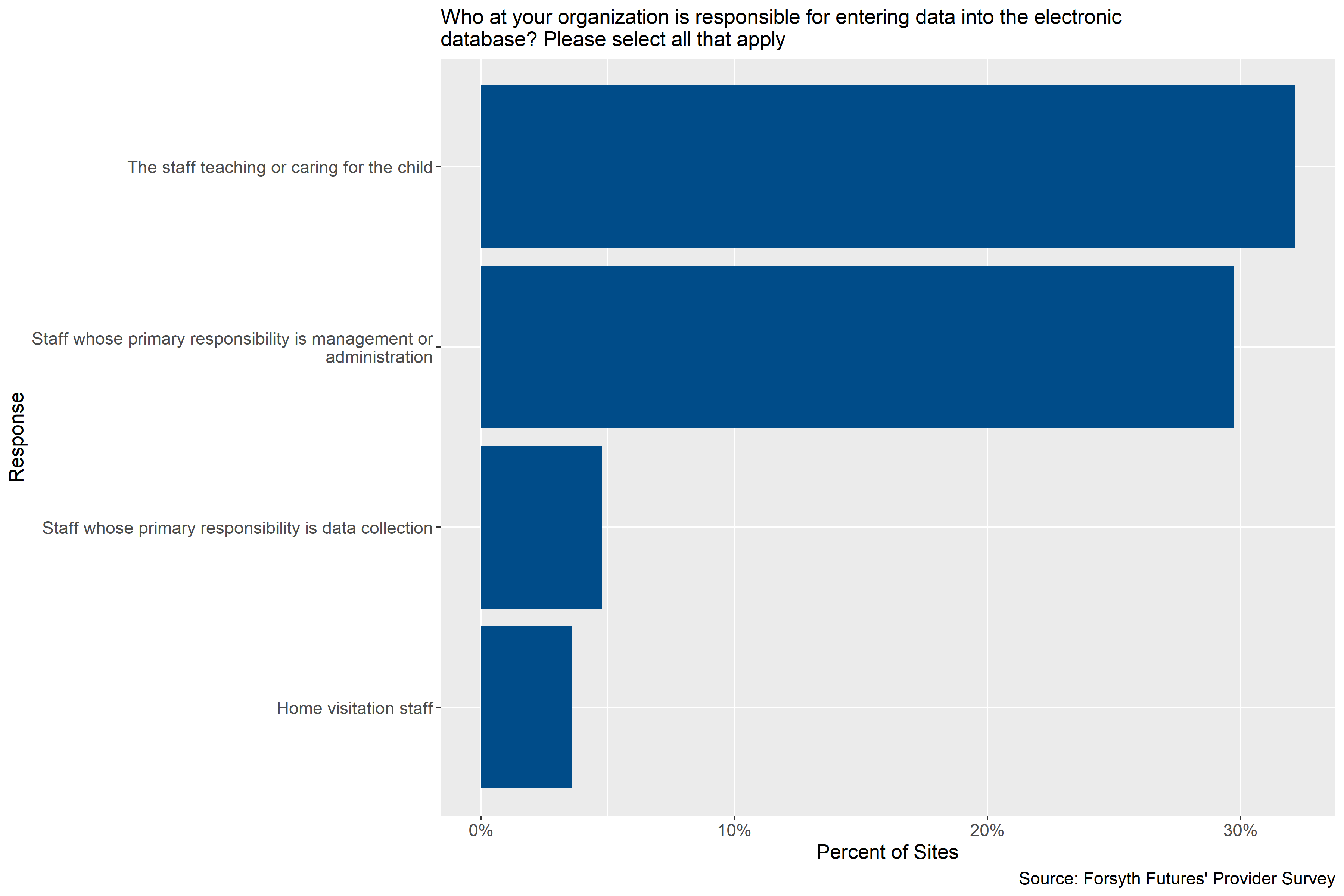
Figure 4.9: Child care staff responsible for entering data into an electronic database (percentage is out of all participating sites)
Figure 4.9 shows that at the child care sites participating in the survey, staff teaching or caring for the child and staff whose primary responsibility is management or administration are staff who are most likely to be responsible for entering data into an electronic database, and a small number of sites use staff whose primary responsibility is data collection. Some participating sites also reported in an open-ended field that requirements were set by a federal government food program and a church, and one respondent noted that the Winston-Salem Forsyth County School system coordinates with Smart Start on a Universal Pre-K application.
4.1.3.2.2 Other Nonprofits and Government Agencies
Survey results show that a variety of people at a given program are involved in entering data into an electronic database(s). The staff range from home visitation staff, nurses and physicians to administrative staff or management. The only staff category not selected by providers was consultants and contractors, but in conversations with providers one provider did note there is a finance and data specialist that assists with data entry. Additionally, two respondents representing a government agency or program noted that social workers are also involved in data entry.
4.1.4 Agencies Setting Data Collection Requirements
This section describes which agencies and organizations currently set data collection requirements for participating child care and pre-k sites and nonprofit, government, and healthcare organizations serving young children.
4.1.4.1 Child Care Providers
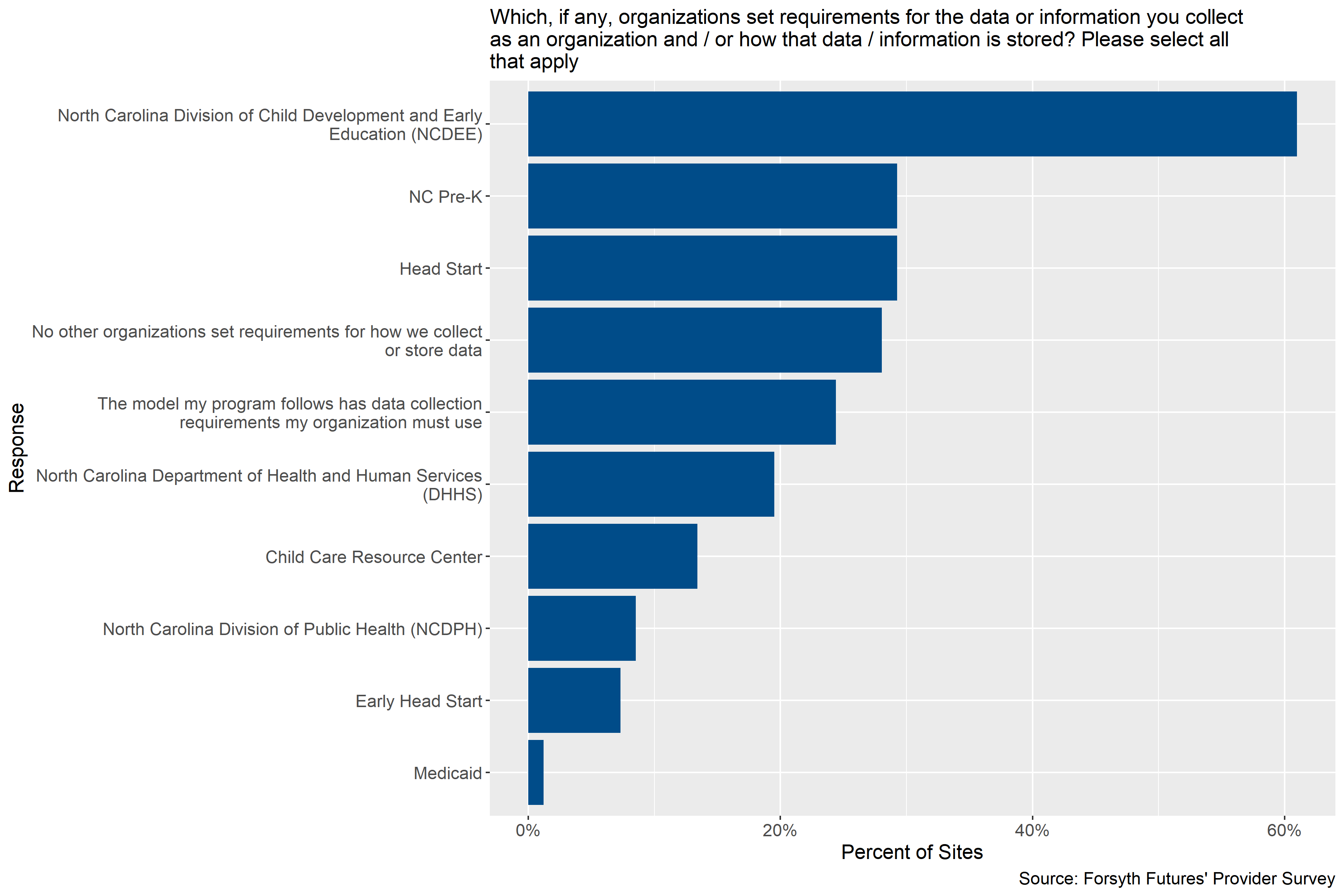
Figure 4.10: Agencies setting data collection and storage requirements for child care providers
Figure 4.10 shows that in cases where other agencies set data collection requirements for child care providers, participating child care sites most often cited the North Carolina Division of Child Development and Early Education (NCDEE) as the organization setting requirements for data collection. About 61% of sites reported requirements for data collection from NCDEE. NC Pre-K and Head Start were identified as agencies setting data collection requirements by about 29% of sites, specific program models by 24% of sites, and the North Carolina Department of Health and Human Services (DHHS) by 20% of sites. About 28% of sites reported that no other organizations set requirements for how data are stored and collected.
4.1.4.2 Other Nonprofits and Government Agencies
About 75% of respondents report that North Carolina’s Department of Health and Human Services (NC DHHS) set data collection or storage requirements. Another 25% and 13% report that Medicaid and United Way, respectively, set requirements. In conversations with providers, 81% reported several other national, state, and local organizations who set data collection or storage requirements not included in the survey. Of those respondents, roughly 44% of them reported additional national entities who have requirements for their program. Examples of national organizations or agencies include the United States Department of Agriculture (USDA), various national programs that oversee the programs in Forsyth County, and the Health Resources Service Administration (HRSA) among others.
State organizations mentioned by respondents included the state WIC program, Blue Cross Blue Shield of North Carolina, and the North Carolina Partnership for Child (NCPC). Clinicians specifically have several national and state bodies overseeing their organization as a whole due to various regulatory and accreditation requirements. Local agencies or organizations identified by respondents include a local hospital system, the local school system, and Kate B. Reynolds Charitable Trust (KBR), and Smart Start of Forsyth County.
4.1.5 Current Data Sharing Practices
This section describes which agencies and organizations participating child care sites and pre-k sites and nonprofit, government, and healthcare organizations serving young children currently share data with and whether they send data to these organizations, receive data, or both.
4.1.5.1 Child Care Providers
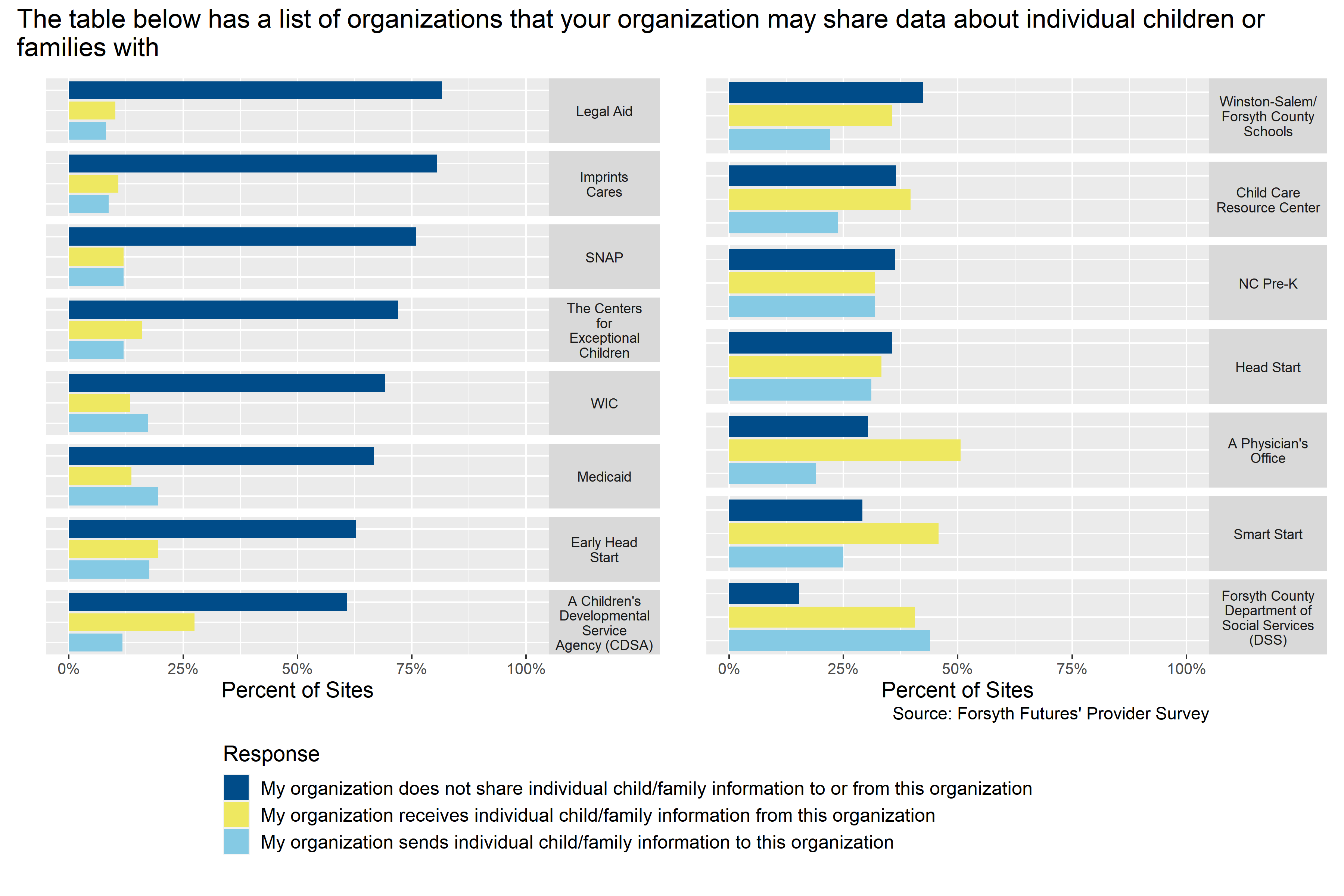
Figure 4.11: Current data sharing practices of child care providers
Figure 4.11 shows that about half of participating child care sites reported sharing or receiving some sort of data from Forsyth County Department of Social Services (DSS), a physician’s office, Smart Start, Head Start, Winston-Salem / Forsyth County Schools, NC Pre-K, and Child Care Resource Center. These agencies were more likely to receive information from than share information with a physician’s office, Smart Start, Winston-Salem Forsyth County Schools, and Child Care Resource Center. And, they were close to equally likely to share or receive information from DSS, Head Start, and NC Pre-K.
4.1.5.2 Other Nonprofits and Government Agencies
Overall, more respondents are not routinely sharing or receiving information on individual families or children from the organizations listed. Of those listed, the Department of Social Services (DSS) and physician offices’ have the highest number of respondents reporting they receive and/or send information about individual children and families. In conversations with providers, there are other organizations or agencies that routinely share or receive information and they include United Way, hospitals, and The Forsyth Promise. Further, sometimes the information shared and/or received is dependent on factors such as family consent to share, necessity, or receiving information indirectly from the organization. For example, one respondent noted that they receive individual information from Medicaid via a third party. Additionally, sometimes the information being shared is more about child care program information. Lastly, certain programs may refer individuals and families to an organization but not directly communicate with the organization. Other programs may directly refer the family to another community provider but it is the family’s responsibility to follow up with the organization.
4.1.6 Current Data Use
This section describes how participating child care and pre-k sites and nonprofit, government, and healthcare organizations serving young children currently use the data they collect and how frequently they create aggregate reports.
4.1.6.1 How Data is Used
4.1.6.1.1 Child Care Providers
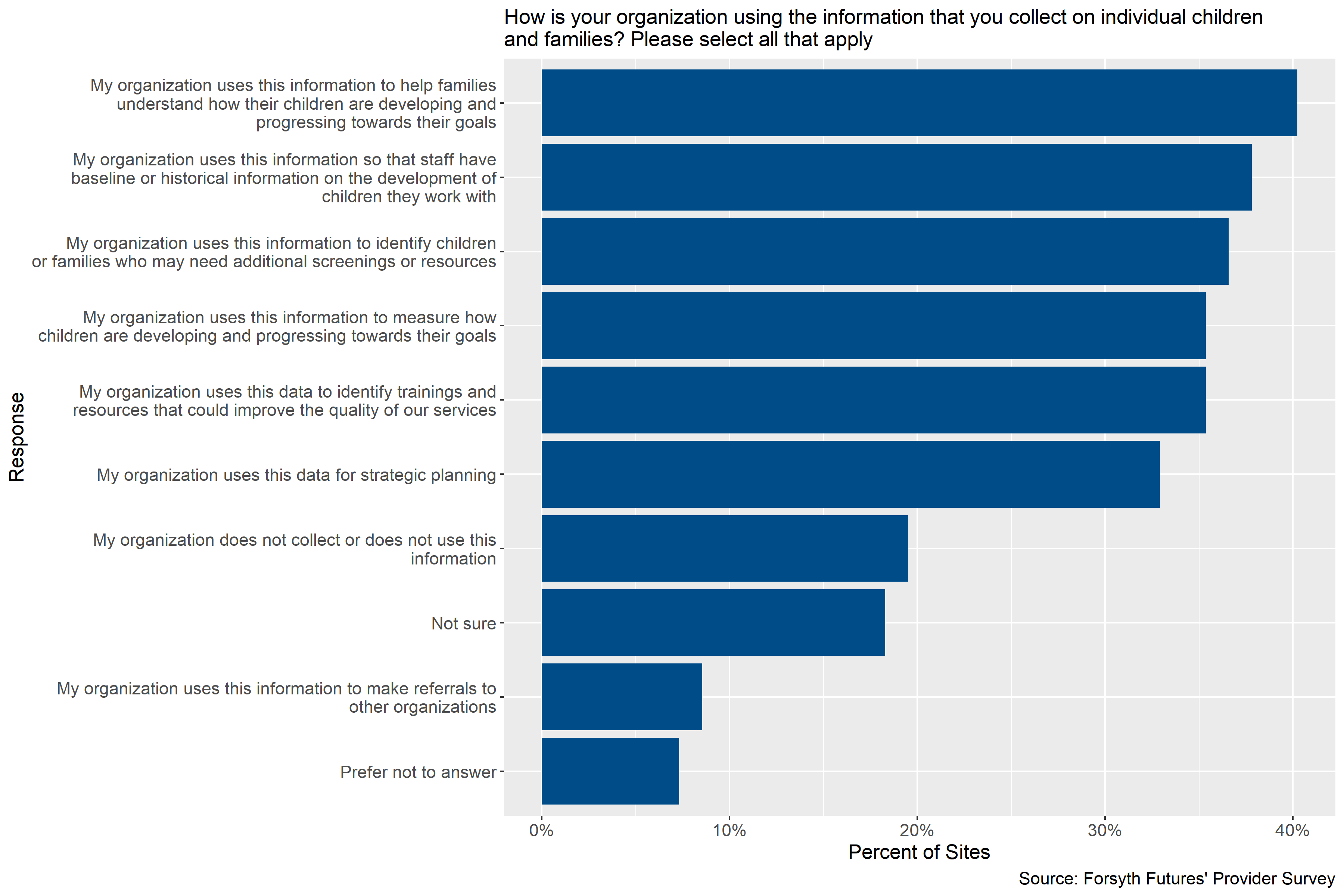
Figure 4.12: How child care providers use data on children and families
Figure 4.12 shows that there was a lot of variety in how child care sites participating in the survey currently use the data they collect. The most common use reported for the data was helping families understand how their children are developing and progressing toward their goals, reported by about 40% of sites. Other common uses for data were providing baseline or historical information about children to staff, identifying children or families that may need additional screening or resources, measuring how children are developing and progressing towards their goals, identifying training that could improve the quality of services, and strategic planning. Each of these uses were reported by 33-38% of sites. Notably, about 18% of organizations were not sure if they used data on individual children and families, and another 20% reported not collecting or not using this data. In open-ended fields of the survey, responding sites reported that they collected or used data as they needed to for operations and to receive payments as well.
4.1.6.1.2 Other Nonprofits and Government Agencies
A plurality of respondents indicate they are using the information they collect on children and/or families in a variety of ways from referring out clients to other organizations to internal organizational use such as strategic planning purposes. Qualitative results suggest that some providers are reporting out to various outside stakeholders relevant to the organization (e.g., county commissioners or Smart Start of Forsyth County) and/or using the information to prioritize the needs of the community members they serve especially in clinical settings.
4.1.6.2 How Frequently Data is Aggregated
4.1.6.2.1 Child Care Providers
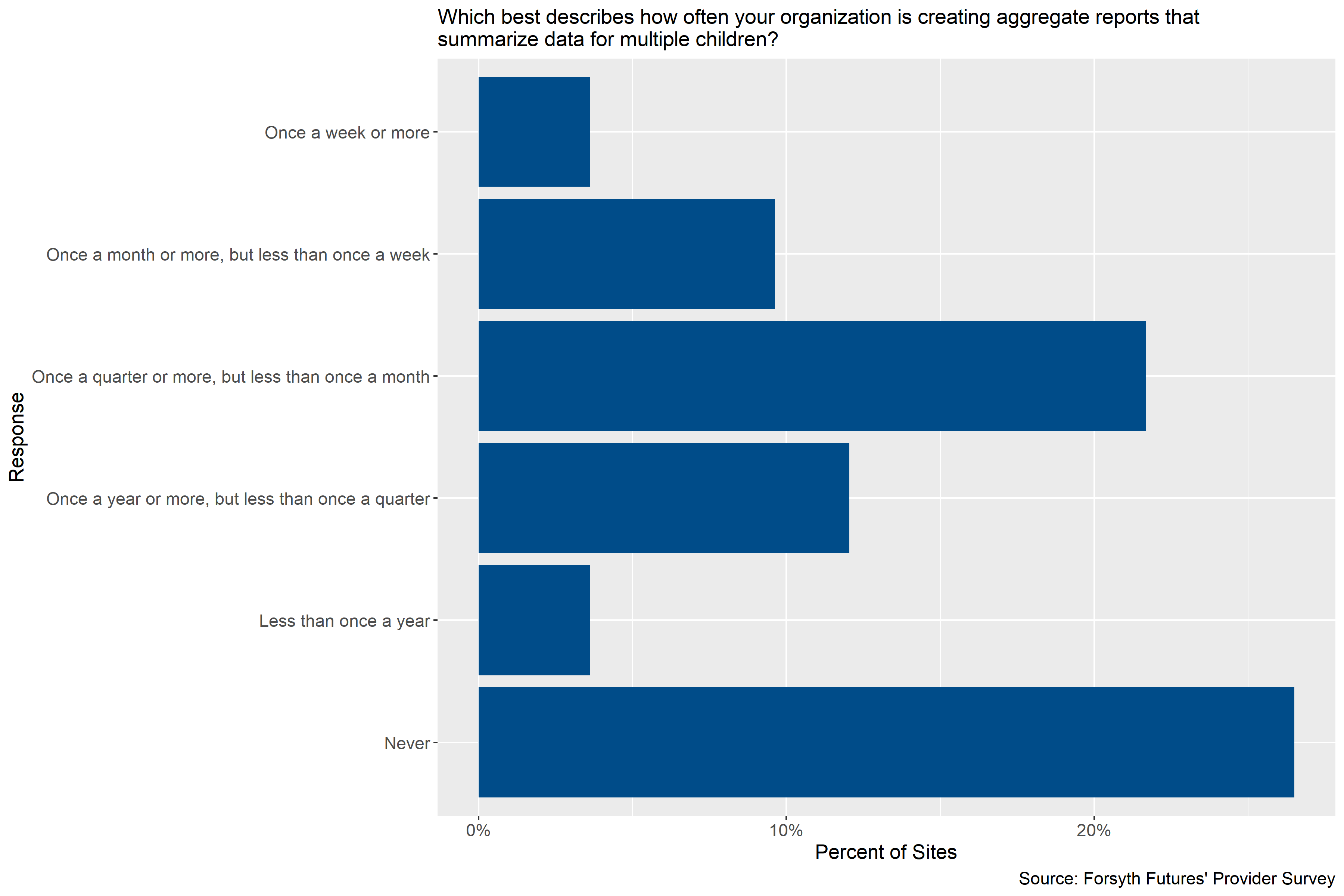
Figure 4.13: How frequently child care providers create aggregate reports
Figure 4.13 shows that child care providers participating in the survey that reported creating aggregate reports most typically produce those reports once a quarter or more, but less than once a month. 10% of sites reported creating aggregate reports once a month or more, but less than once a week, and 12% once a year or more, but less than once a quarter, respectively. And, some sites reported creating reports more or less frequently. Notably, more than a quarter of sites participating in the survey reported that they never created aggregate reports.
4.1.6.2.2 Other Nonprofits and Government Agencies
Most providers (about 69%) report creating aggregated reports on the children/families they serve once a quarter or more, but less than once a month. Two providers that represent a governmental agency or program do not produce any aggregate reports. In conversations with providers, one provider noted that the state produces their own aggregated reports that sometimes the organization uses to inform best practices while another provider noted that they occasionally receive one-off requests for reports from various community stakeholders.
4.2 Interest in a Data Hub
This section describes participating child care and pre-k sites’ and nonprofit, government, and healthcare organizations’ potential interest in participating in a data hub. It includes information about how likely organizations would be to participate in different data sharing activities, what factors would increase the likelihood of participation on a data hub, and information organizations would like to but do not currently have on hand.
4.2.1 Likelihood of Participation
This section describes participating child care and pre-k sites’ and nonprofit, government, and healthcare organizations’ potential interest in participating in a data hub by examining how likely they would be to participate in different types of data sharing that could be facilitated by a data hub.
4.2.1.1 Child Care Providers
Figure 4.14: How likely child care providers are to participate in a data sharing hub
Figure 4.14 shows that majority of participating child care provider sites reported being likely or very likely to participate in a data sharing hub by their organization collecting more information about children that are served to improve services provided by the organization as a whole, to collect more information to improve services for individual children, and to receive summary reports on the early childhood system as a whole that do not include individual child data to help inform the organization’s planning or grant writing. A little more than a third of responding sites reported being likely or very likely to participate in any of the other ways described in the survey and shown in Figure 4.14. Notably, about 40% of respondents reported not being sure about how likely they would be to share information their organization had collected or to receive information on individual children. About 16% of respondents reported that they were “Unlikely” or “Very unlikely” to share information on individual children with outside organizations to inform their work with those children and with outside evaluators so that they could measure the impact of programs.
In open-ended fields of the survey, a couple providers noted that they would need to consult their corporation’s guidelines or their legal department about how or if they could be involved. One respondent noted that gathering data could be positive for helping families and children reach their highest capacity, but that collecting the data would increase the work load for teachers, which would take time and energy away from children. When asked if there was anything else that they would like to share about their organizations’ likelihood of participating in a data hub, one responding site responded that they were “very much interested”.
4.2.1.2 Other Nonprofits and Government Agencies
A majority of respondents indicated that they would be likely or very likely to receive or view information on individual children or aggregate reports on young children as a whole. But, less than half of respondents indicated they would be interested in sharing information on individual children that they gathered with other organizations or outside evaluators. Additionally, respondents as whole appear to be likely as opposed to unlikely to collect more information to improve services for the population they serve.
In conversations with providers, many indicated that sharing and receiving information would be dependent on privacy laws and family consent. Respondents expressed concern with sharing any information about individuals given various HIPAA and other privacy constraints. Thus, participation would be contingent on ensuring privacy agreements, such as memorandum of understandings (MOUs), are in place. Additionally, two providers noted that there would have to be some agreement among funders on how the data is captured, used, and secured (e.g., data security).
4.2.2 Factors Facilitating Participation
This section describes factors that participating child care and pre-k sites and nonprofit, government, and healthcare organizations serving young children reported as factors that would encourage them to participate in a potential data hub.
4.2.2.1 Child Care Providers
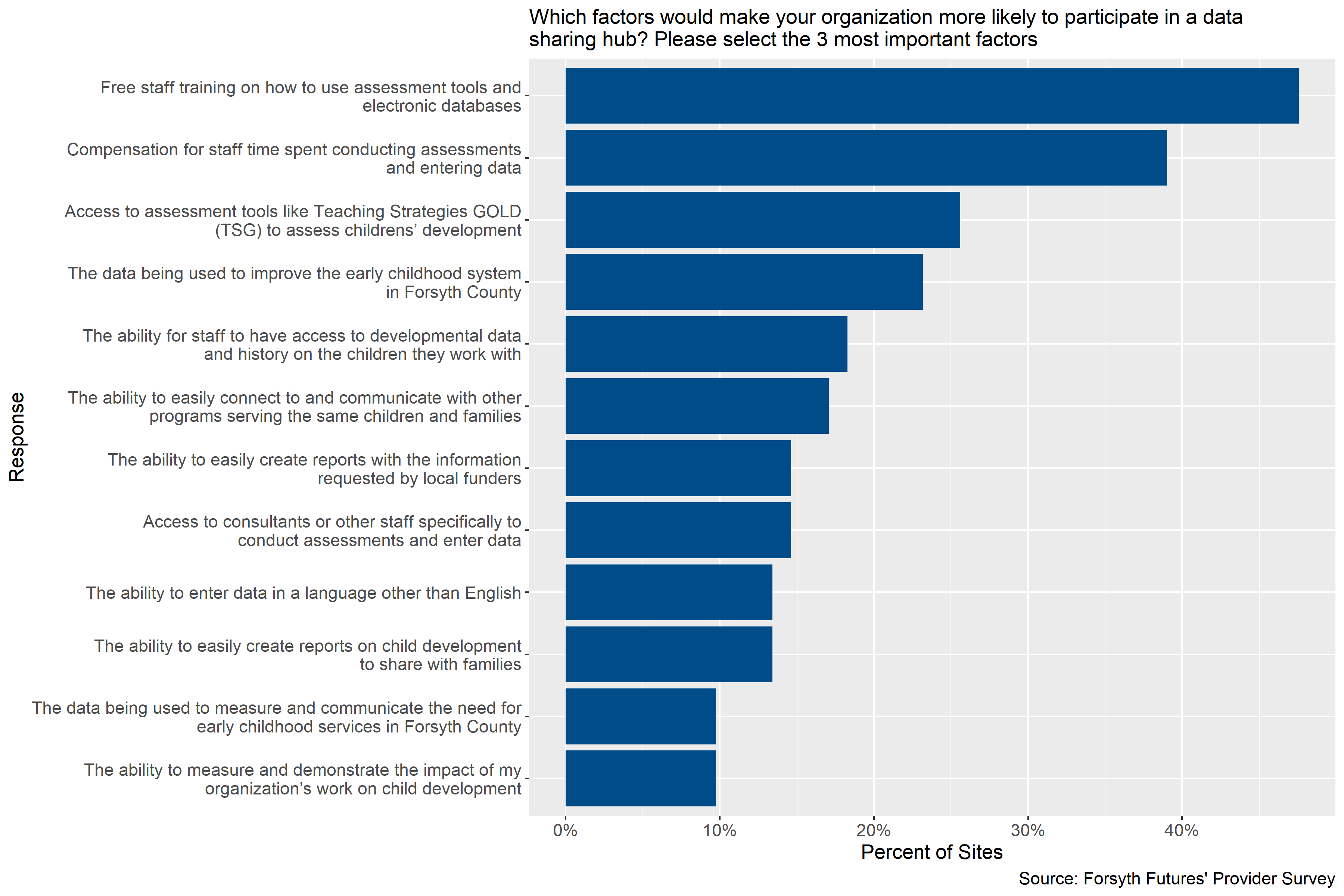
Figure 4.15: Factors making child care sites more likely to participate in a data sharing hub
Figure 4.15 shows that participating child care sites gave a variety of answers to the question, “Which factors would make your organization more likely to participate in a data sharing hub?”. The most common response was “free staff training on how to use assessment tools and electronic databases” followed by “compensation for staff time spent conducting assessments and entering data”, with 48% of sites and 39% of sites giving those answers, respectively. About a quarter of sites reported that access to assessment tools like Teaching Strategies GOLD (TSG) to assess children’s development and the data being used to improve the early childhood system in Forsyth County.
In open-ended fields, two respondents identified permission or advise from their corporate office or legal department as something that would facilitate participation. One respondent noted that participation would not be beneficial to their program, another noted that it should be optional and private, and another noted that they would be interested in collecting this information if there was one place - like an app or a website - to collect it and enter it electronically. When asked if there was anything else they would like to share about participating in a data hub, one respondent noted that they were not sure if a data hub was the best way to serve providers at this time unless it was a secure hub of potential employees and their history.
4.2.2.2 Other Nonprofits and Government Agencies
About 56% of respondents reported that if the data sharing hub made it easy to connect and communicate with other programs serving the same children and families, then their organization would be more likely to participate. Roughly 38% of respondents also reported that a data sharing hub with the ability to measure and demonstrate organizational impact on child development would increase their organizations likelihood. Lastly, 31% of respondents said that their organization would need compensation for staff time to administer assessments, the ability to easily create a report for local funders, and that the data is used to measure and communicate the need for early childhood services in Forsyth County to make increase their organizations likelihood of participating in data sharing hub.
4.2.3 Information Needed by Organizations
This section describes information that could potentially be provided by a data hub that participating child care and pre-k sites and nonprofit, government, and healthcare organizations serving young children would like to access but do not currently have access to.
4.2.3.1 Child Care Providers
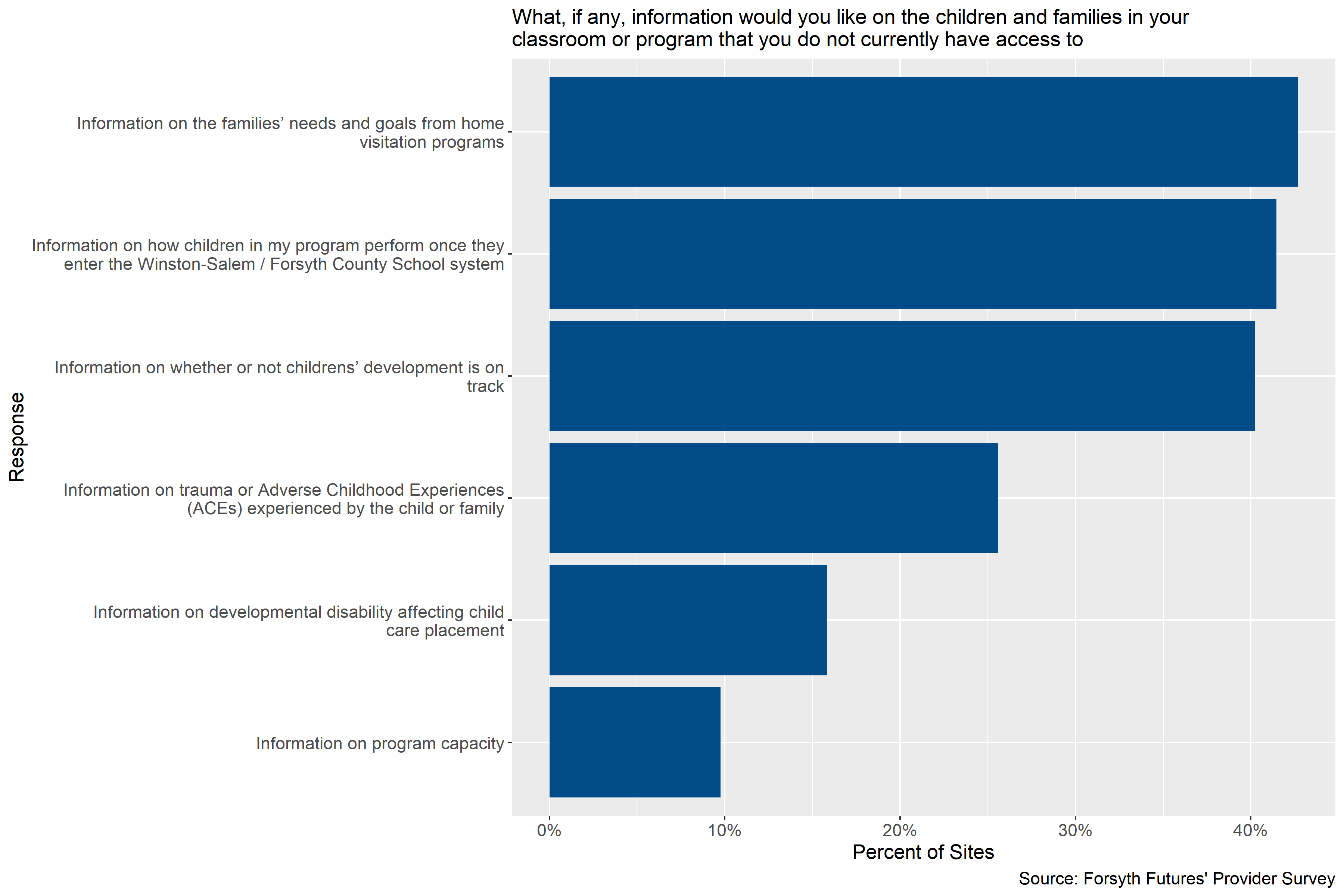
Figure 4.16: Information child care sites would like but do not have access to
Figure 4.16 shows that between 40% and 43% of participating child care sites listed information on families’ needs and goals from home visitation programs, information on how children in their program perform once they enter the school system, and information on whether or not children’s development is on track as information that they would like on children and families that they do not currently have access to. In the open-ended fields for this question, one respondent noted that there was no information that they would like and did not have access to and one site noted that their organization is small and communicates regularly with families.
4.2.3.2 Other Nonprofits and Government Agencies
Respondents varied in what information they would like to know that they currently do not have access to but the most frequent response, with about half of respondents, was wanting information on the trauma or Adverse Childhood Experiences (ACEs) experienced by the child or family. Additionally, of the two of three responses requesting additional information on program capacity were from clinical programs.
Other information providers would like to know not captured in the table are the community resources the family is utilizing or what other programs the family is enrolled in or received services from, screening or assessment results, and more health information.
4.3 Resources and Supports Needed
This section describes the resources and supports that participating child care and pre-k sites and nonprofit, government, and healthcare organizations serving young children reported needing to be able to collect additional data on individual children and families, conduct and collect information from additional assessments and screenings, and participate in a data hub.
4.3.1 For Data Collection
This section describes the resources and supports that participating child care and pre-k sites and nonprofit, government, and healthcare organizations serving young children reported needing to be able to collect additional data on individual children and families and conduct additional assessments and screenings. It also describes how frequently organizations reported needing these resources and supports.
4.3.1.1 Information About Children and Families
4.3.1.1.1 Frequency of Needing Supports
4.3.1.1.1.1 Child Care Providers
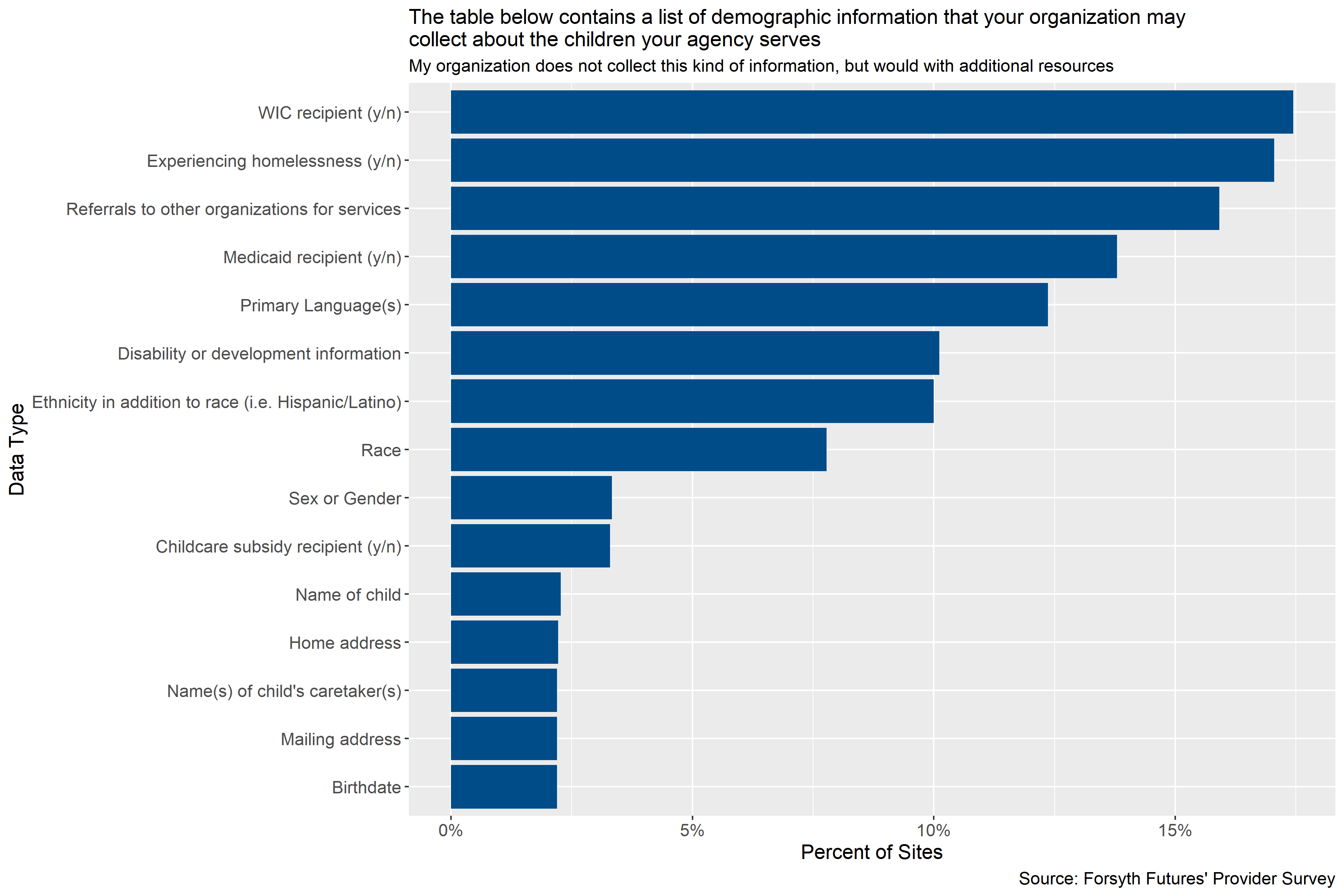
Figure 4.17: Information about children child care providers would need additional resources to collect
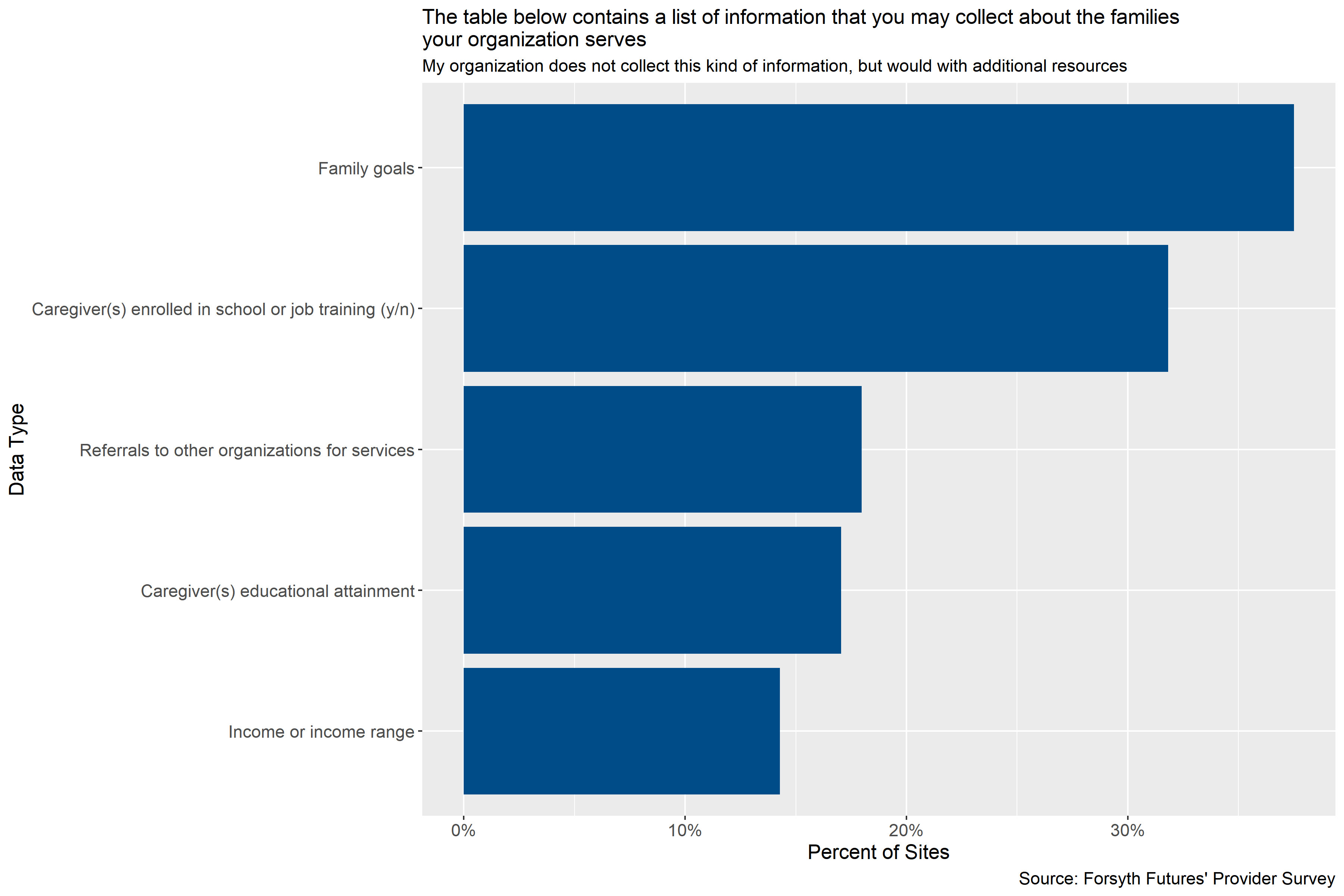
Figure 4.18: Information about families child care providers would need additional resources to collect
Figure 4.17 and Figure 4.18 show that more participating child care sites reported needing support to collect additional information on families than children. The data that the most sites would be willing to collect with support are family goals (38% of sites), whether or not caregivers are enrolled in school or job training (32%), and referrals to other organizations for services (18%).
4.3.1.1.1.2 Other Nonprofits and Government Agencies
Of the nine respondents that selected at least one of the response options in the survey on the minimum resources needed to collect various demographic data, the most frequent response with four responses was that they would not need additional resources or they are already collecting the information. The next most common response was compensation for staff time.
4.3.1.1.2 Supports Needed
4.3.1.1.2.1 Child Care Providers
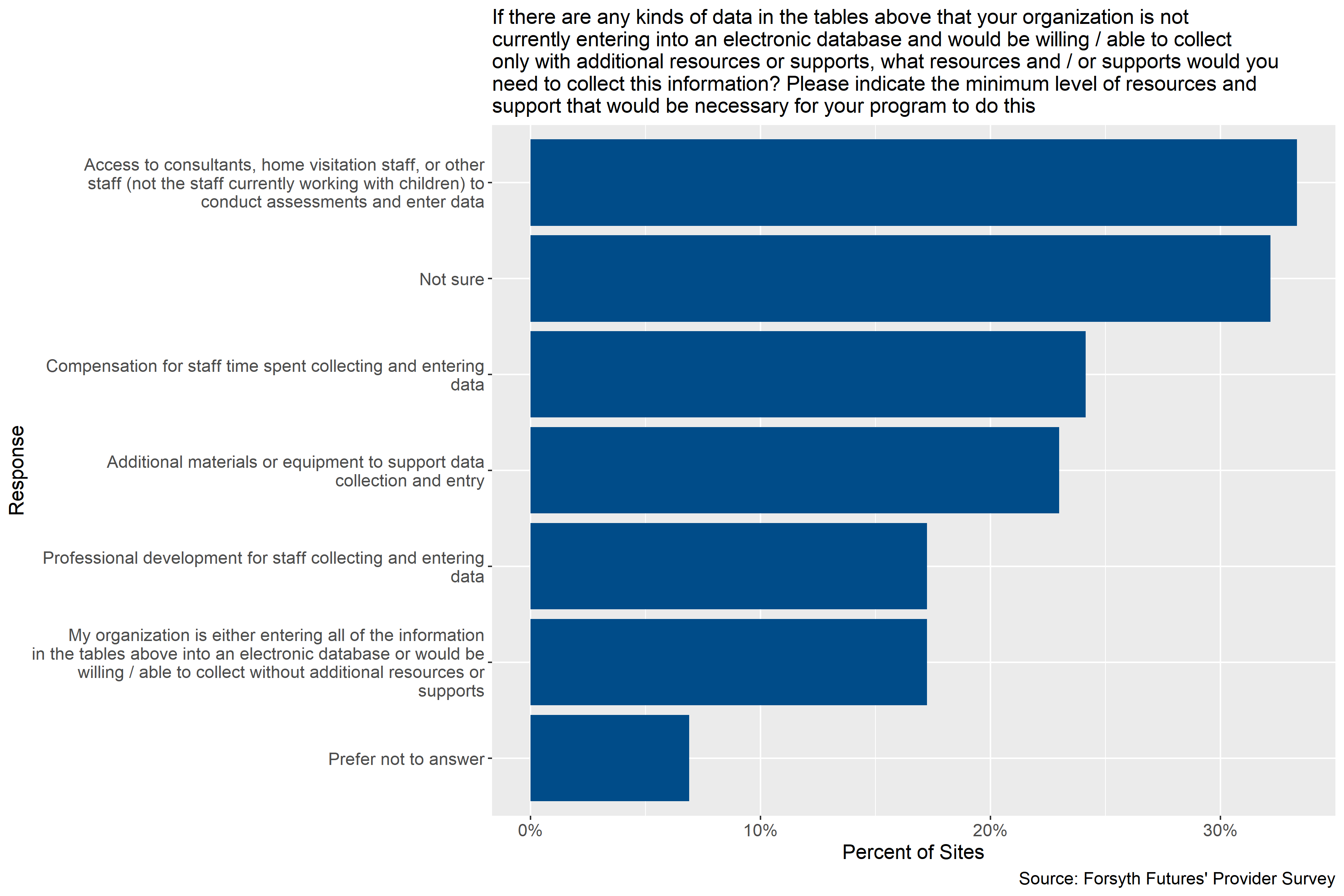
Figure 4.19: Supports child care providers need to collect and enter information on families and children
Figure 4.19 shows that the most common support that participating child care sites reported they would need to be able to collect the information on children and families described in Figure 4.1 and Figure 4.2 and enter it into an electronic database is access to consultants, home visitation staff, or other staff (not currently working with children) to conduct assessments and enter data. About 33% of participating sites reported needing this support. The next most common supports required, reported by about 24% and about 23% of participating sites respectively, were compensation for staff time spent collecting and entering data and additional materials or equipment to support data collection and entry. Notably, about 17% of participating sites reported that their organization was either already collecting all of the information listed in Figure 4.1 and Figure 4.2 or they would be willing and / or able to collect this information without additional resources or supports, and about 32% of sites reported not being sure about the kinds of supports they would need.
In open-ended fields of the survey, three participating respondents noted that they would potentially need an additional staff person or additional staff time / capacity. Two respondents indicated that they were prohibited from entering or sharing specific information, especially without authorization, and one respondent indicated that they did not have an electronic database. About 7% of participating sites reported needing some other kind of support that was not listed in Figure 4.19 above.
4.3.1.1.2.2 Other Nonprofits and Government Agencies
About 63% of respondents provided comments about the minimum resources needed for their ability to collect additional demographic data they are not currently collecting. Half of those responses were centered around time, capacity, or privacy constraints. One respondent noted that they would need additional staff since they are social workers and not necessarily data specialists. Further, another respondent said that they may be able to collect additional information but it would be hard to share given privacy laws. The other half of respondents reported that some of the information they are not currently collecting is because it is not relevant to the program. Data collection and/or storage is often what is required for the program.
4.3.1.2 Assessments and Screenings
4.3.1.2.1 Frequency of Needing Supports
4.3.1.2.1.1 Child Care Providers
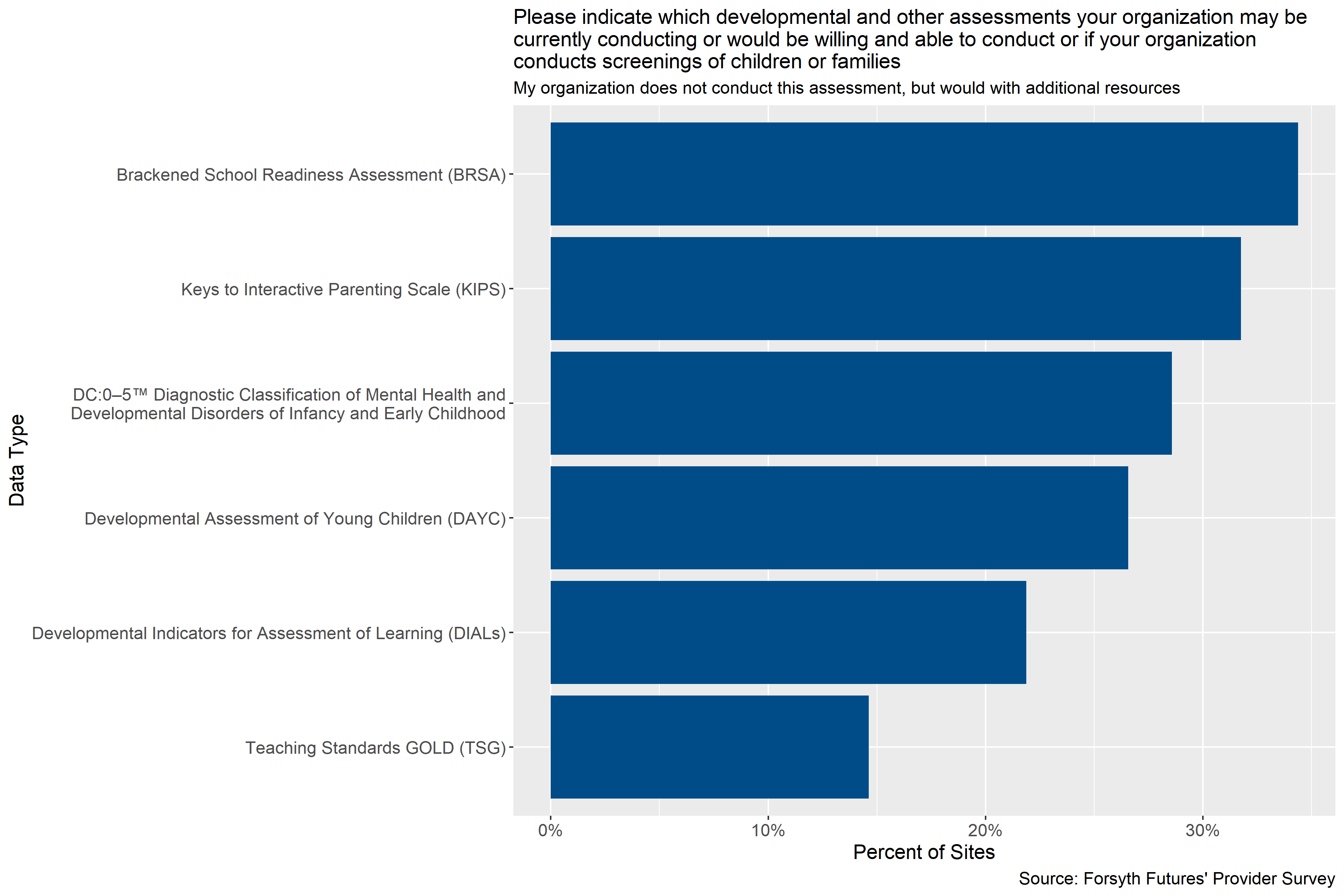
Figure 4.20: Percent of sites that are not currently conducting assessments but would be willing to with additional supports or resources
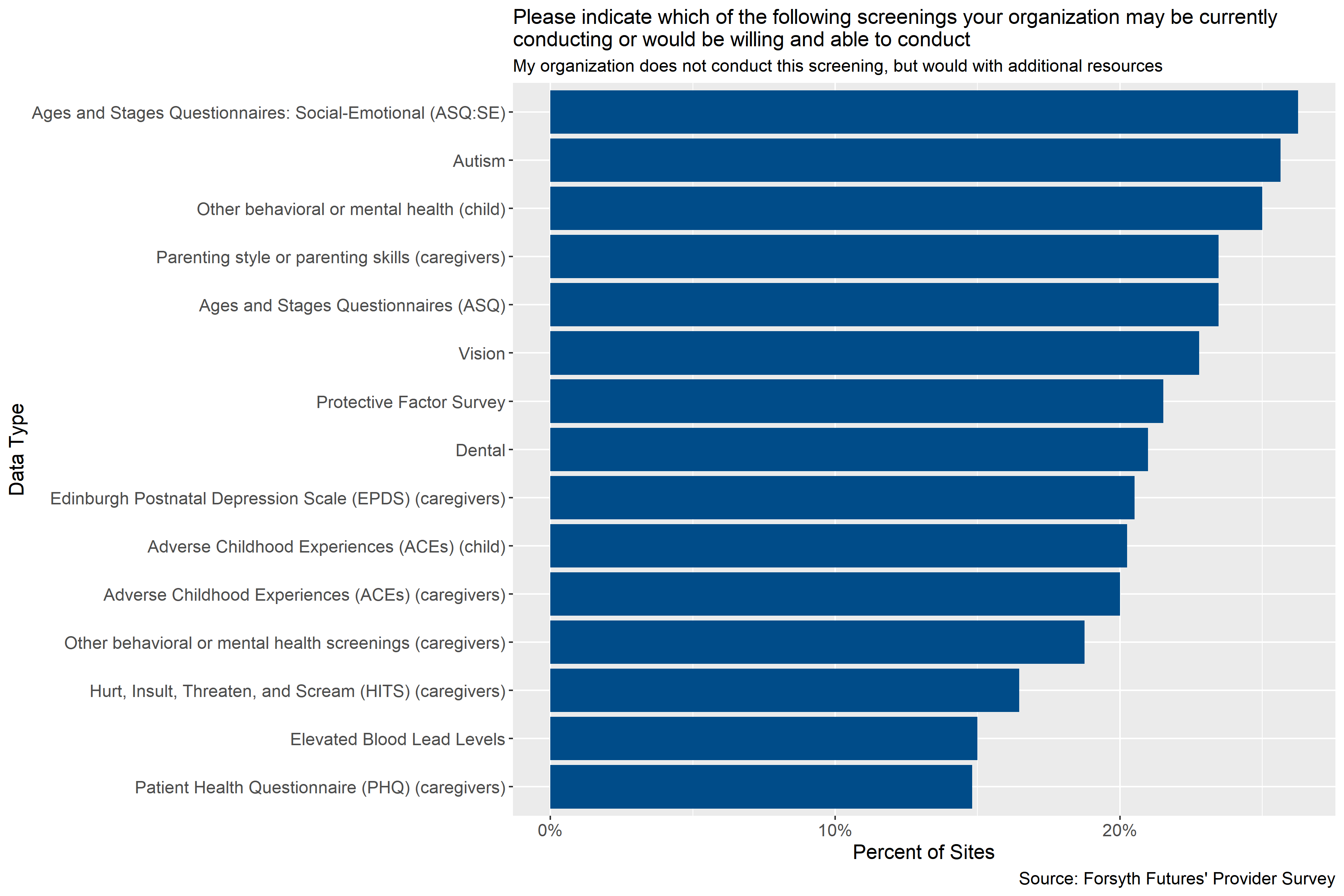
Figure 4.21: Percent of sites that are not currently conducting screenings but would be willing to with additional supports or resources
Figure 4.20 and Figure 4.21 show that across all of the screenings and assessments included in the survey between 15% and 34% of participating sites reported that they were not currently conducting the screenings and assessments but would be willing to with additional supports and resources.
4.3.1.2.1.2 Other Nonprofits and Government Agencies
The most frequent response to what minimum supports are needed to administer various assessments and screenings was for staff time entering data followed by staff time for conducting assessments and no additional resources that would allow their organization to conduct and enter data from screenings/assessments.
4.3.1.2.2 Supports Needed
4.3.1.2.2.1 Child Care Providers
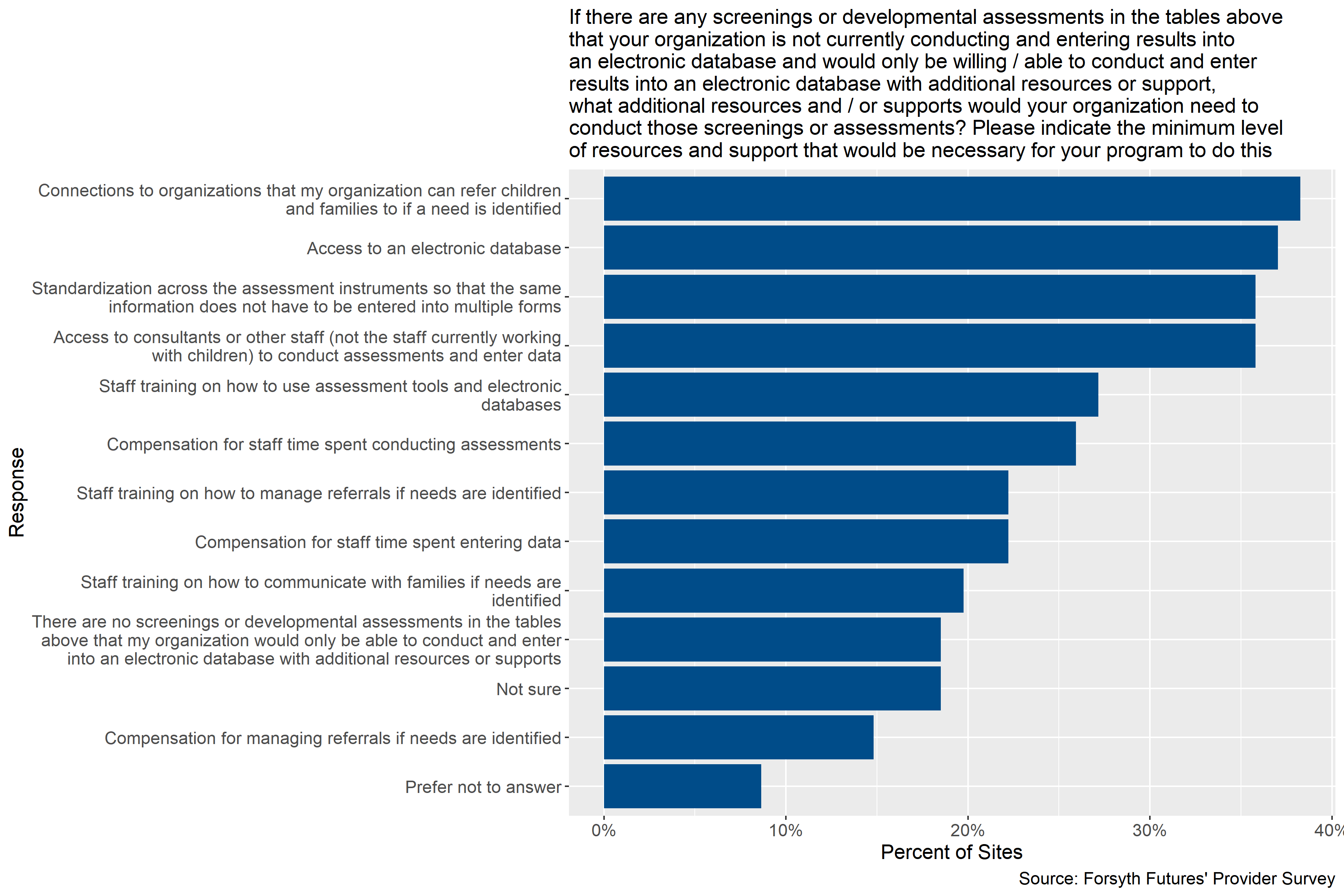
Figure 4.22: Supports child care providers need to conduct and enter screenings and assessments
Figure 4.22 shows that the most common supports participating child care sites reported needing to be able to conduct the assessments and screenings listed in Figure 4.3 and Figure 4.4 were connections to organizations for referrals if needs are identified, access to an electronic database, standardization across the assessment instruments so that the same information does not have to be entered into multiple forms, and access to consultants or other staff (not the staff currently working with children) to conduct assessments and enter data. About 36% to 38% of sites reported needing these supports. The next most common supports needed were staff trainings on assessment tools and the electronic database, compensation for staff time spent conducting assessments and entering data, and staff training on managing referrals and communicating findings to parents, reported by 19% to 27% of sites. About 19% of sites reported that there were no screenings or assessments listed in Figure 4.3 and Figure 4.4 that they would only be able to conduct and enter into an electronic database with additional resources or supports, and about 19% of sites reported not being sure.
In open-ended fields of the survey, one participant reported not being sure because of their organization’s corporate guidelines and another respondent indicated that they have always been able to find resources for needs for families as those needs arise.
4.3.1.2.2.2 Other Nonprofits and Government Agencies
In conversations with providers, concern was expressed around staff time/capacity of administering screenings/assessments and data entry. Also, sometimes national organizations set the parameters of what screenings/assessments and data is collected. Lastly, a couple of respondents mentioned that screenings/assessments are not applicable to their program goals or their specific program is referral focused.
4.3.2 For Data Hub Participation
This section describes the resources and supports that participating child care and pre-k sites and nonprofit, government, and healthcare organizations serving young children reported needing to be able to participate in a data hub and how frequently they reported needing these supports.
4.3.2.1 Child Care Providers
4.3.2.1.2 Supports Needed
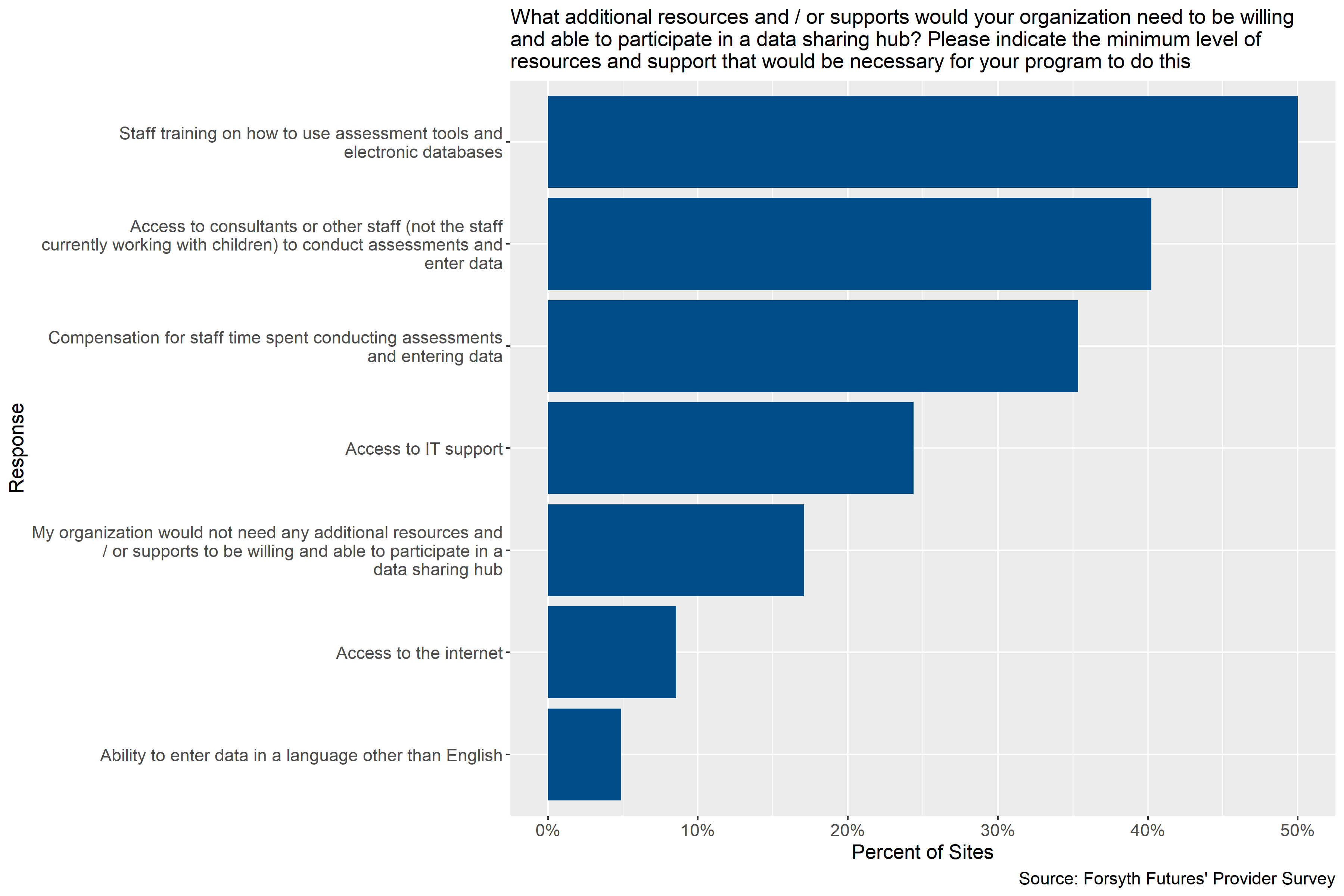
Figure 4.23: Supports child care providers need to participate in a data hub
Figure 4.23 shows that the most common supports that participating child care providers reported needing to participate in a data hub were: staff training on how to use assessment tools and electronic databases (reported by 50% of participating sites), access to consultants or other staff (not the staff currently working with children) to conduct assessments and enter data (40%), and compensation for staff time spent conducting assessments and entering data (35%). About a quarter of participating sites reported that they would need access to IT support, and slightly less than 10% reported needing access to the internet. About 17% of participating sites reported not needing any additional resources and / or supports.
In open-ended fields of the survey, two participants noted that they would need permission from their boards or corporate governance to participate, with one respondent noting that participation would not work for them.
4.3.2.1.3 Other Nonprofits and Government Agencies
Survey results show that half of respondents reported that they would need access to IT support and staff training on how to use assessment tools and electronic databases for their participation in the data hub. About 38% of respondents reported they would need compensation for staff time spent on data collection and entry. In conversations with providers, approximately 33% of respondents noted that their participation in a data sharing hub would be dependent on additional factors not listed in the survey. These factors include being able to demonstrate value to individuals a given program serves, needing permission from various organizations and agencies involved in programs (e.g., NC DHHS, local school system etc.), and the size and scope of the data sharing hub. Some respondents felt the data sharing hub description was too vague so they were unsure about the complexity of the hub.
4.4 Barriers
This section describes the barriers to data hub participation reported by participating child care and pre-k sites and nonprofit, government, and healthcare organizations serving young children. It includes information on the barriers reported to collecting additional information on children and families, conducting additional screenings and assessments, and data hub participation more generally.
4.4.1 Collecting Data
This section describes the barriers to collecting additional information on children and families and conducting additional assessments and screenings reported by participating child care and pre-k sites and nonprofit, government, and healthcare organizations serving young children.
4.4.1.1 Information on Children and Families
4.4.1.1.1 Child Care Providers
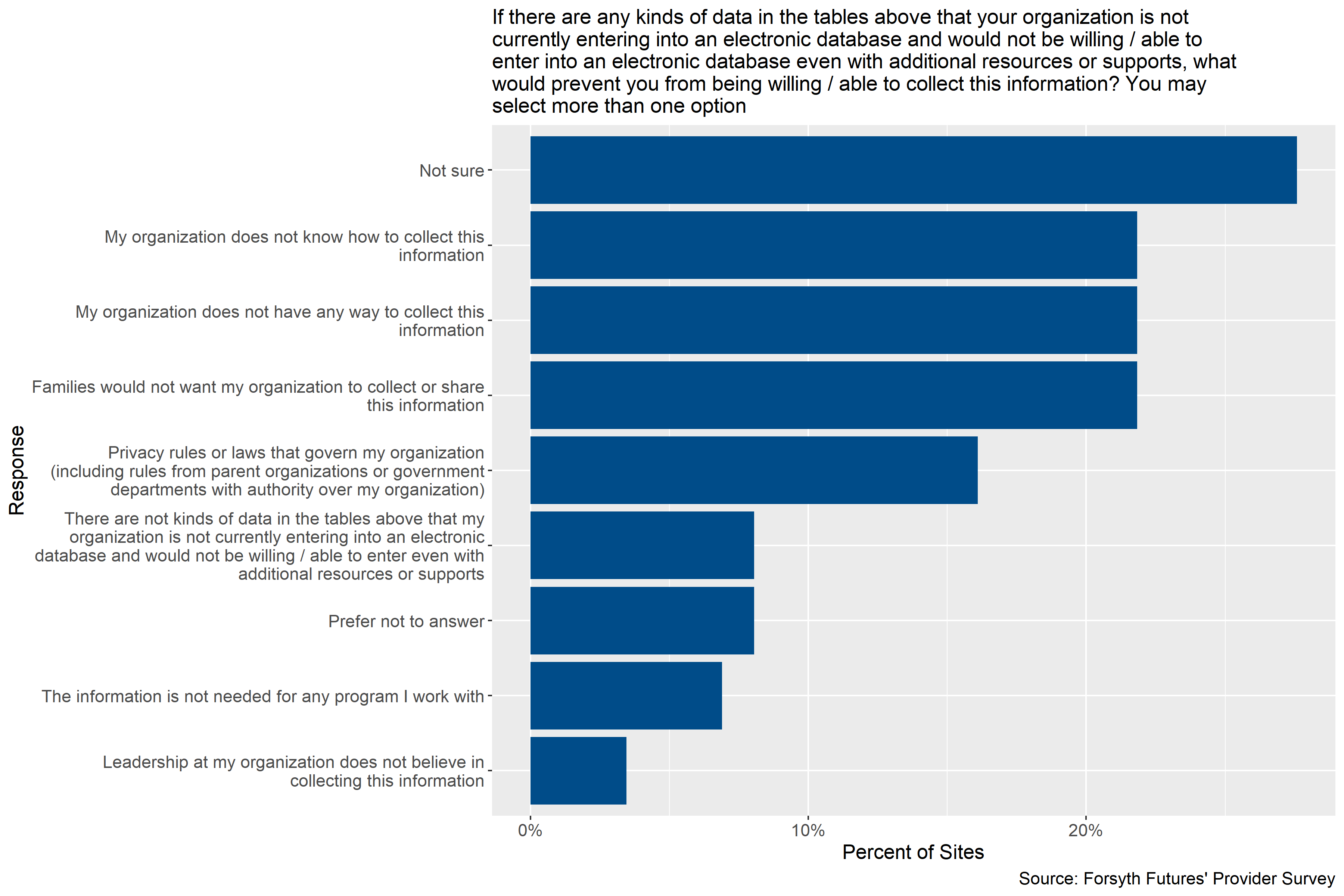
Figure 4.24: Child care providers’ barriers to collecting data on children and families
Figure 4.24 shows that the when asked if there were any kinds of data listed in Figure 4.1 or Figure 4.2 that providers are not currently entering into an electronic database and would or could not enter into an electronic database even with additional resource or supports, what would prevent them from doing so, the most common response provided by participating child care sites was “Not sure” (reported by 28% of sites). The next most common responses were that organizations do not know how to collect the information, organizations do not have any way to collect this information, and that families would not want this information collected or shared which were all reported by 22% of sites participating. About 16% of sites reported that privacy rules or laws that govern their organization were a barrier to participation.
In open-ended fields of the survey, three respondents indicated that they collect some of the information described in Figure 4.1 or Figure 4.2 but that they do not have or do not enter the data into an electronic database. Two sites reported that parents would not be comfortable with their personal information being shared, with one respondent noting that would particularly be the case if parents do not know how the information is being used or stored or whether or not the information is anonymous. And, one respondent reported that their board would need to make decisions about participation.
4.4.1.1.2 Other Nonprofits and Government Agencies
In addition to program applicability, other barriers to collecting various data elements include time and/or capacity constraints, privacy concerns from the families they serve, data storage capability, and needing buy-in from both families and institutional leaders.
4.4.1.2 Screenings and Assessments
4.4.1.2.1 Child Care Providers
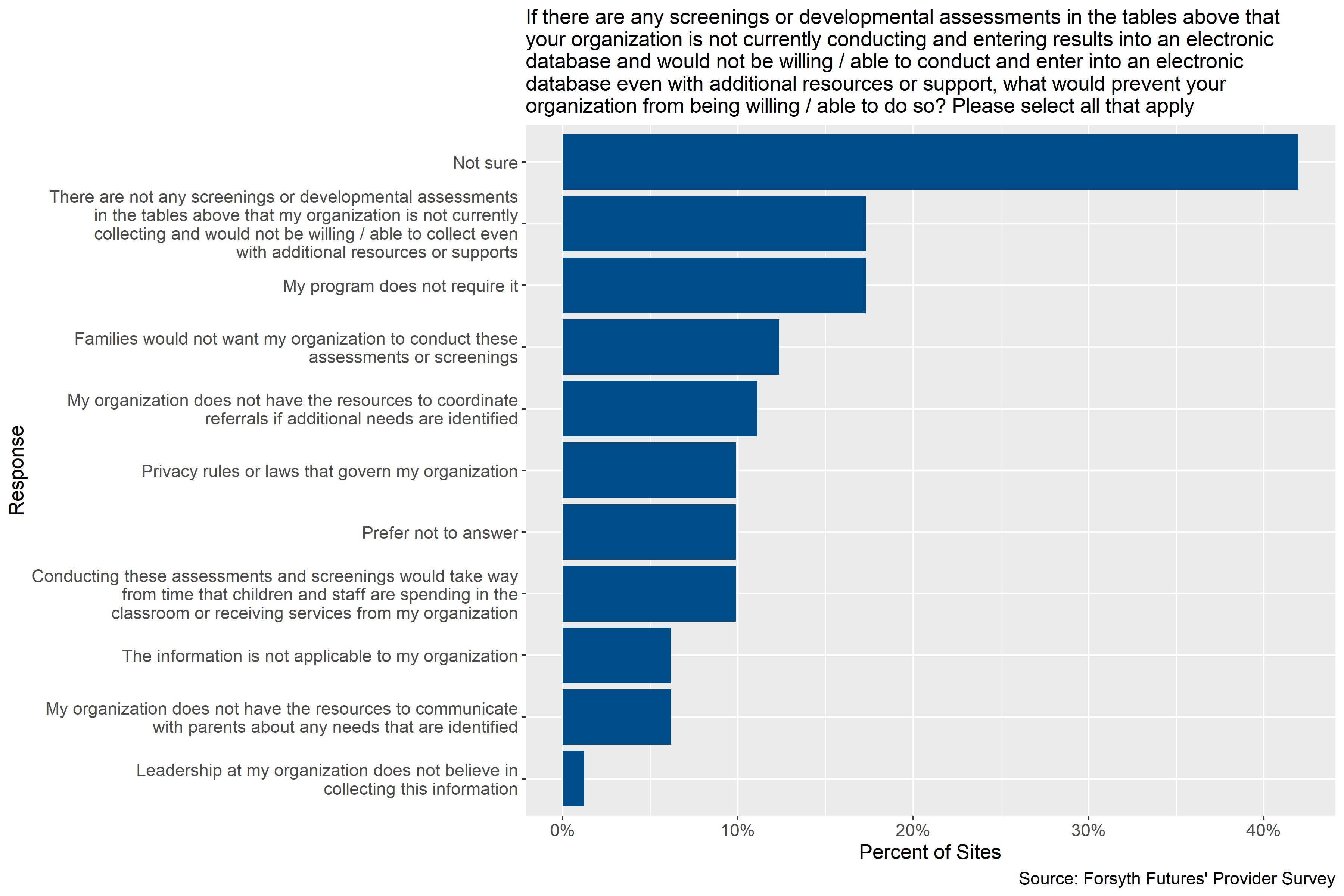
Figure 4.25: Child care providers’ barriers to conducting screenings and assessments
Figure 4.25 shows that when asked if there were any screenings or assessments listed in Figure 4.4 and Figure 4.3 that providers are not currently conducting and entering into an electronic data base and could or would not do so even with additional resources or supports, the most common response given was “Not sure” (given by 42% of participating sites) followed by providers reporting that there were not any screenings or assessments listed in Figure 4.4 and Figure 4.3 that they would not or could not conduct (17%). The next most common responses were that the sites program does not require it (17%).
In open-ended fields of the survey, the only response given was that the respondent was unsure because their response would have to be based on their corporate guidelines.
4.4.1.2.2 Other Nonprofits and Government Agencies
Some of the reasons for providers not being willing/able to administer and manage screenings/development assessments ranged from information not being applicable to the program and time/capacity constraints. As noted elsewhere, national organizations set the parameters of what screenings/assessments and data is collected. Additionally, one respondent emphasized that a child’s information (such as their protected health information) would need to be protected so they could not be individually identified. Another respondent worried that Smart Start of Forsyth County would force providers to have more data collection requirements and an additional data storage system.
4.4.2 Data Hub Participation
This section describes the barriers to participating in a data hub described by participating child care and pre-k sites and nonprofit, government, and healthcare organizations serving young children.
4.4.2.1 Child Care Providers
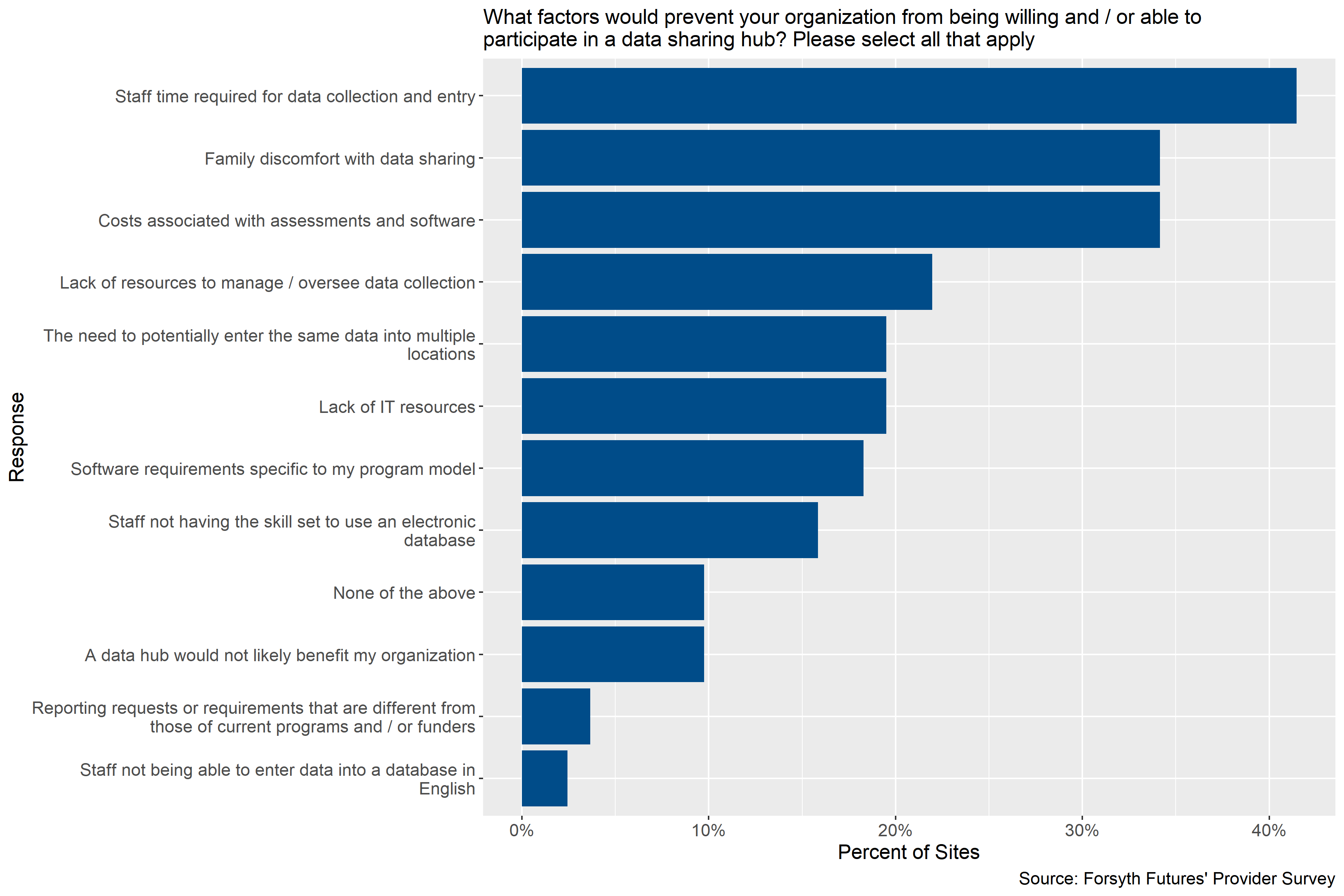
Figure 4.26: Factors preventing child care providers from participating in a data sharing hub
Figure 4.26 shows that the most common factors that would prevent participation in a data sharing hub reported by participating child care sites were: staff time required for data entry (reported by 41% of sites), family discomfort with data sharing (34%), and costs associated with assessments and software (34%).
In open-ended fields of the survey, one respondent indicated that their organization’s legal department would have to answer this question, and another reported that they were not sure if their company would take the opportunity to invest.
4.4.2.2 Other Nonprofits and Government Agencies
Respondents were asked about what factors would prevent their organization from being willing or able to participate in a data sharing hub. The most frequent response was for staff time required for data collection and entry followed by family discomfort with sharing data and potential need to enter the same data in multiple locations. Qualitative data suggests, as noted elsewhere, that permission from various entities that work with or fund the program is also needed. Additionally, although no one selected in the survey that the hub would not benefit their program, a respondent did note in conversation that their specific program would not benefit from a data sharing hub given the population they serve (infants).
4.5 Other Considerations from Stakeholders Surveyed
This section describes the comments provided by participating child care and pre-k sites and nonprofit, government, and healthcare organizations serving young children when asked if there was anything that they thought should be considered when planning a potential data hub.
4.5.1 Child Care Providers
When asked if there were any additional things that Smart Start should consider while exploring what an early childhood data hub might look like, the only open-ended response given by a participating child care site was “no”, but that the respondent wanted to be kept informed of developments.
4.5.2 Other Nonprofits and Government Agencies
Six respondents provided additional feedback on what they think Smart Start of Forsyth County should know about any potential development of a data sharing hub. Two respondents noted that any conversations need to involve the community to get their perspectives while one of those two argued that the data sharing hub should not just be for Smart Start of Forsyth County services. Additionally, a concern was expressed about not duplicating services and that there needs to be information or a demonstration of what is being done well already. Other respondents noted that resources will be needed if they want data and that Smart Start of Forsyth County should look at what services and data entry costs.
Two respondents expressed hesitation about any participation in or development of a data hub. One noted their reservation since they were involved with the previous Smart Start of Forsyth County attempt at a centralized data sharing hub. They were explicitly concerned that the community would not be receptive to having their data shared among multiple providers and that clients may share less information if they think their information will be available to various stakeholders. This concern was tied to high risk groups (e.g., substance users, undocumented residents) specifically and that any kind of trust built could be impacted. Another respondent reported that the community does not have an informational needs gap but rather a financial resource gap in the community.