Chapter 10 Medical Microbiology
A host is a larger organism that supports the growth and development of a smaller organism. Parasites, on the other hand, are organisms that:
- Live on or within an organism and are metabolically depenedent (i.e., they get their food from their host) on their hosts.
- They harm their host in some way (e.g., bacteria, protozoa, helminths, fungi, and even viruses).
10.1 Host-Parasite Relationships
An infection is a parasite that grows and multiplies wihtin or on a host - this may or may not result in an infectious disease
A disease - on the contrary - is a change of state in health in which part of or all parts of the host is incapable of carrying their normal functions.
A pathogen is a microbial parasitic organism that causes an infectious disease. Primary pathogens cause disease via direct interaction with the healthy host - an opportunistic pathogen is a pathogen that may be part of the normal flora and causes disease when it gains access to other tissue sites or when the host is immunocompromised.
The pathogenicity of a parasite is its tendency to cause disease.
10.1.1 What impacts host-parasite outcomes?
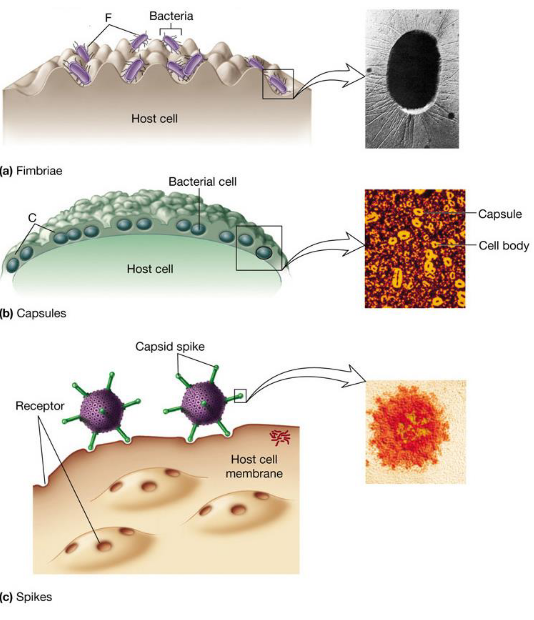
Figure 10.1: Virulence Factors in Microorganisms
The number of organisms present, the virulence of the pathogen (e.g., whether or not it has capsules, pili, and what kind of toxins it produces), and the host’s defense and degree of resistance all play a part.
10.2 Progression of an Infectious Disease
The signs of an infectious disease are objective changes that can be directly measured or observed. Symptoms are subjective changes experienced by the patient - this is similar to a syndrome: a set of characteristic signs and symptoms.
10.2.1 Course of an infectious disease
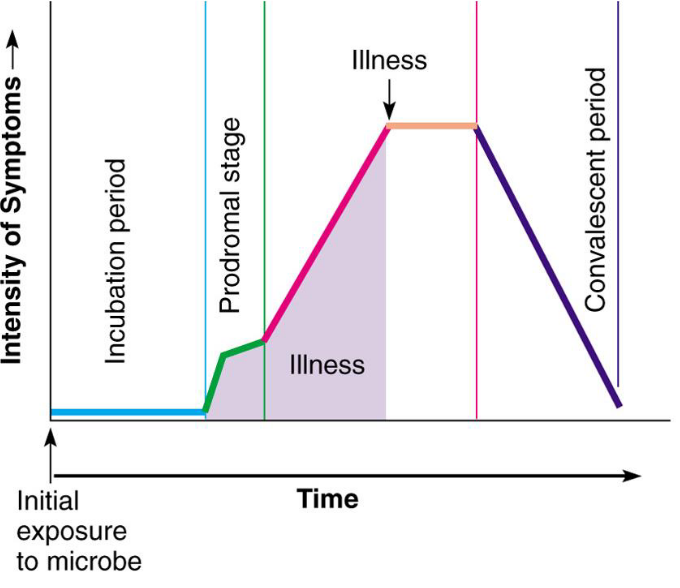
Figure 10.2: Progression of an Infectious Disease
The incubation period refers to the period of entry (of the pathogen) before symptoms and signs appear.
The prodromal stage refers to the onset of signs and symptoms; however, the onset is usually not clear enough for a proper diagnosis.
The period of illness is a period of time where the illness is the most severe - the signs and symptoms characteristic with the disease develop here.
Convalescence occurs when signs and symptoms start to disappear.
The latent stage is when the pathogen is not transmissable - no symptoms are present in the host (e.g., herpes, syphilis).
10.3 Source or Reservoir of a Disease
The source is the location from which the pathogen is transmitted to the host (whether it is direct, indirect, animate, or inanimate).
The period of infectivity is the time during which the the source is infectious or is disseminating the organism.
A source is different from a reservoir: the natural environmental location where the pathogen is normally found. Sometimes, the source of a pathogen is the reservoir of the pathogen.
A carrier is an infected host who is a potential source for infecting others. There are several types of carriers:
- Active carriers have overt, clinical case of the disease.
- Convalescent carriers have recovered from the disease, but they continue to harbor large numbers of the pathogen.
- Healthy carriers harbor the pathogen, but they are not ill themselves (i.e., they are asymptomatic).
- Incubatory carriers incubate the pathogen in large numbers, but they are not yet ill.
It is important to note that numerous diseases are zoonoses: most animals act as a reservoir of parasites and transmit infectious diseases to humans directly or indirectly (e.g., rabies, SARS, MERS, etc). Arthropod vectors are organisms that spread disease from one host to another.
10.3.1 Transmitting Pathogens
There is evidence that suggests correlation between transmission modes and virulence:
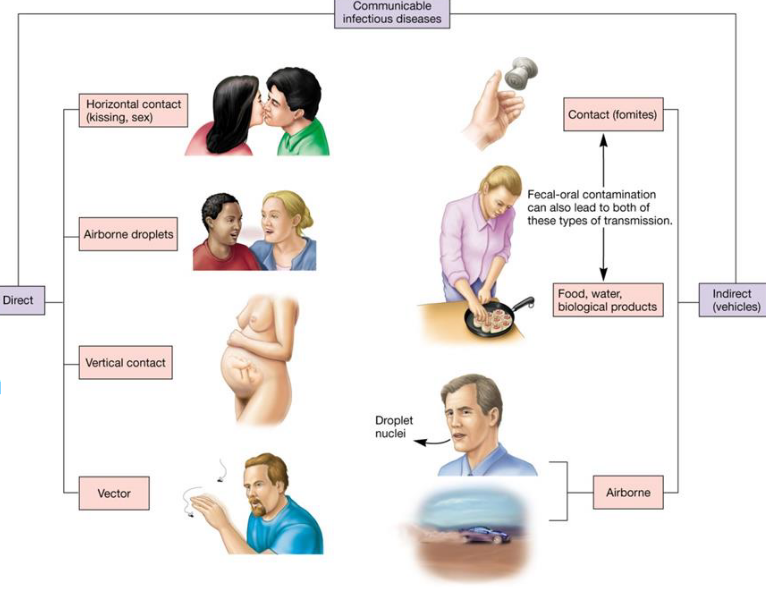
Figure 10.3: Modes of Transmission
Direct contact is usually less virulent; vector-borne diseases are highly virulent. Parasites that are outside the host are also more virulent.
10.4 Modes of Transmission and Infections
There are four main modes of transmission:
- Airborne
- Contact
- Vehicle
- Vector-borne
10.4.1 Airborne transmissions
These are transmitted through the air over time and distance. Respiratory droplets are larger than 5 - 10 micrometers in diameter.
Droplet nuclei, on the contrary, are about 1 to 4 micrometers in diameter - they remain airborne for a longer period of time and can also travel longer distances. They are transmissable via coughing, sneezing, talking, and coughing
10.4.2 Contact transmission
This refers to physical surfaces coming into contact of each other or the touching of a source / reservoir of pathogens.
Direct contact between two people can include kissing, touching, and sexual activity.
Indirect contact involves an intermediate (e.g., eating utensils, bedding, etc.); the intermediate is often inanimate.
Larger particles (i.e., greater than 5 micrometers in diameter) usually travel less than one meter.
10.4.3 Vehicle transmission
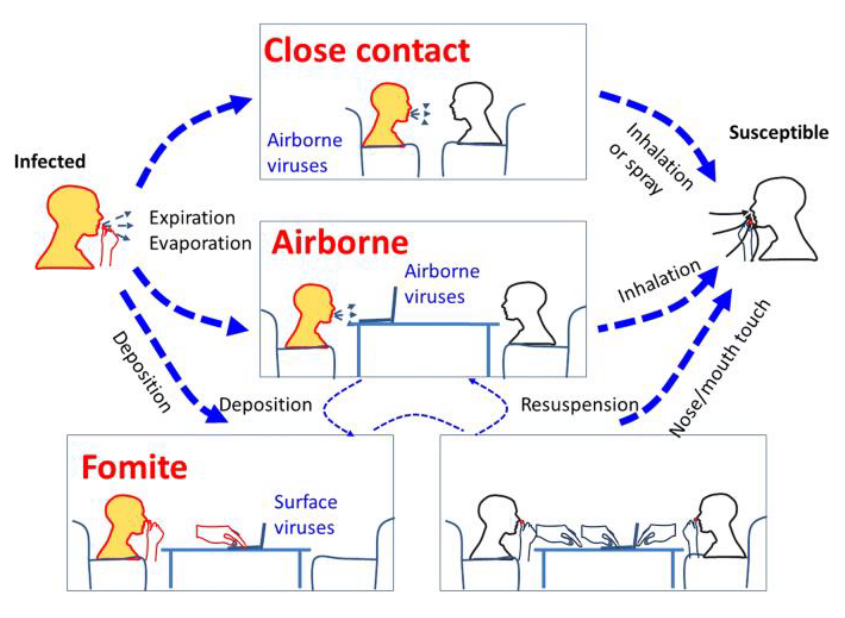
Figure 10.4: Types of Vehicle Transmissions
A vehicle is an inaminate object that is involved in pathogen transmission. A common vehicle transmission occurs when a single vehicle spreads pathogens to multiple hosts.
Fomites are common vehicles: surgical instruments, bedding, and eating utensils are all examples.
10.4.4 Vector-borne transmission
This is an external mechanism that involves the passive carriage of the pathogen on the body of the vector. There is no growth of the pathogen during transmission (e.g., shigella on fly feet from feces to food).
Internal transmission is also posisble: harborage transmission occurs when the pathogen does not undergo changes within the vector. This is in contrast to biologic transmission: pathogens do undergo changes within the vector (e.g., the plague or malaria).
10.4.5 Growth rates
All pathogens must find favorable conditions inside their host cells. Extracellular pathogens grow outside cells in blood and tissue fluids.
Intracellular pathogens, on the contrary, grow and multiply within cells. Facultative intracellular pathogens are able to grow within or outside cells - obligate intracellular pathogens, on the contrary, only grow when inside cells.
10.4.6 Host susceptibility
There are two main factors for determining the susceptibility of a host to an organism:
- Its defense mechanisms
- The pathogenicity of a pathogen
Nutrition, genetic predisposition, and stress also play a role in host susceptibility to infection.
10.4.7 Exiting the host
If the pathogen is to be perpetuated, it must eventually leave its host. There are two ways of doing so:
Passive escape occurs during excretion in feces, urine, droplets, blood, saliva, and desquamated cells.
Active escape occurs during the movement of a pathogen to the portal of an exit (e.g., parasitic helminths).
10.5 Patterns of Infectious Disease within a Population
A communicable disease is a disease that can be transmitted from one host to another (e.g., the common cold).
Epidemiology is a branch of science that determines the frequency and distribution of disease - for instance, whether or not an outbreak is sporadic or whether or not an outbreak is endemic or pandemic.
10.5.1 Two types of epidemics
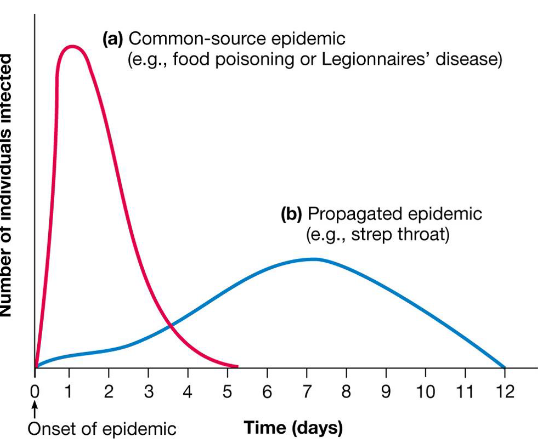
Figure 10.5: Two Types of Epidemics
Common source epidemics result from a single, common contaminated source (e.g., food).
Propagated epidemics result from the introduction of a single infected individual into a susceptible population (where the disease is propagated to others).
Surveillance is also necessary to recognize and measure an infectious disease in a population. Surveillance methods include:
- Gathering information on the development and occurrence of a disease
- Colalting and analyzing infection data
- Summarizing findings
- Selecting control methods
10.5.2 Herd Immunity
This is the resistance of a population to the spread or an infection of an infectious organism because of the immunity of a large percentage of the population:
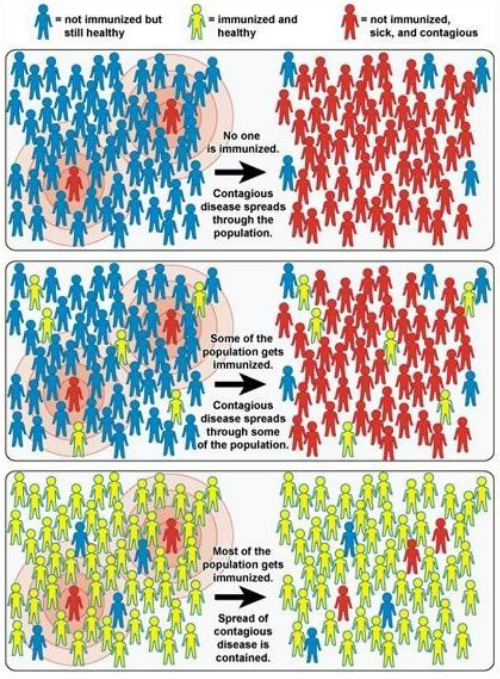
Figure 10.6: Herd Immunity Depicted
It is important to note that herd immunity is altered by the introduction of new, susceptible individuals into the population and also changes in the pathogen.
Antigenic shift refers to a major change in the antigenic character of the pathogen (e.g., the influenza virus). Antigenic drift refers to smaller antigenic changes.
10.5.3 Emerging infectious diseases (EIDs)
The northeastern portions of the US, western Europe, Japan, and southeastern Australia are all hot spots of emerging spots of infectious diseases - some of these “infectious diseases”are novel whereas some are old.
It is interesting to note that many of these “infectious diseases” are zoonotic: they emerged from an animal, but crossed the species barrier to infect humans (e.g., Nipah virus, SARS-CoV-2, Zika virus, etc).
10.5.3.1 Why are EIDs on the rise?
Some reasons include the following:
- A larger world population
- More international travel
- Habitat disruption of reservoirs
- Microbial evolution
- Bad public infrastructures
- Climate change
- Social unrest
- Changes in food processing techniques
- Changes in human behavior and technology
- Medical practices that encourage immunosuppression
10.5.4 Nosocomial infections
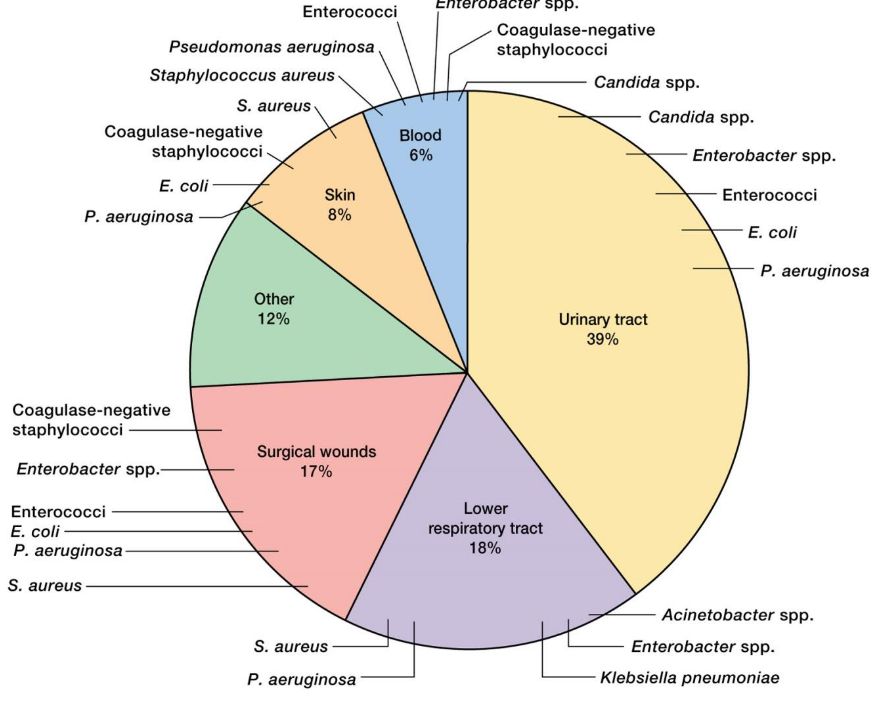
Figure 10.7: Proportion of Nosocomial Infections and Causative Bacteira
These are hospital-acquired infections; the pathogens in a nosocomial infection develop within a hospital or some other clinical care facility and are subsequently acquired by patients while they are in the facility.
About 10% of all hospitals will acquire a nosocomial infection.
Urinary tract infections (i.e., UTIs) are the most common - there are also many antibiotic-resistant hospital strains of pathogenic bacteria.
10.6 Antimicrobial Resistance
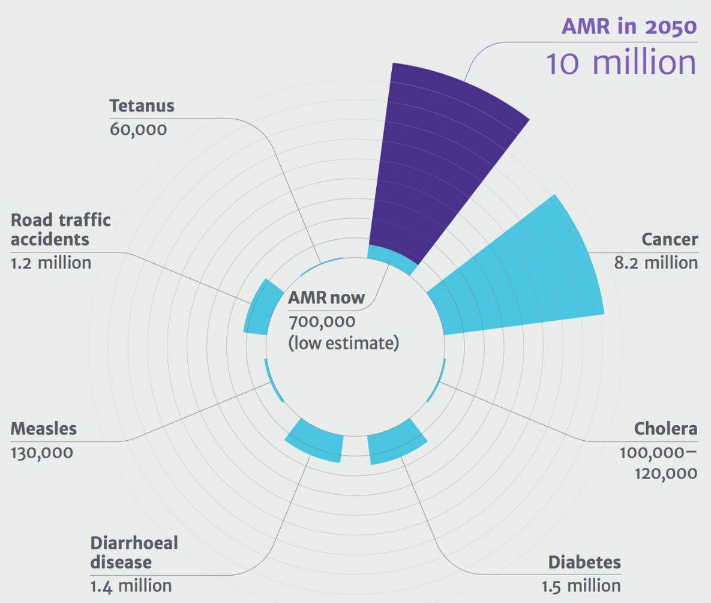
Figure 10.8: Antibiotic Resistance Deaths
It is estimated that about 10 million people will die from drug-resistant infections each year by 2050 unless some form of action is taken.
10.6.1 Clostridioides difficile

Figure 10.9: C. diff. Infographic
These are a class of anaerobic, spore-forming gram-positive bacteria that are found in the intestine of some healthy individuals.
While their population is kept in check by other normal intestinal microbiota (i.e., colonization resistance), excessive antibiotic use eliminates normal microbiota allows C. difficile to overgrow.
10.6.1.1 Virulence factors
C. difficile multiplies and produces toxins in the process, causing inflammation, diarrhea, fever, nausea, and cramping in the process. Antibiotic-associated diarrhea (i.e., AAD) is the most common cause of diarrhea in hospitalized patients.

Figure 10.10: Pseudomembranous Colitis
In severe cases, pseudomembranous colitis may result: a viscous collection of inflammatory cells, dead cells, necrotic tissue, and fibrin obstructs the passage of food through the small intestine.
Toxic megacolon is a phenomenon that results in the death of intestinal tissue. While this is rare, this is also life-threatening.
While C. difficile is treated with antibiotics, recurrence of the bacteria is common!
10.6.2 Carbapenem-resistant Enterobacteriaceae (CRE)
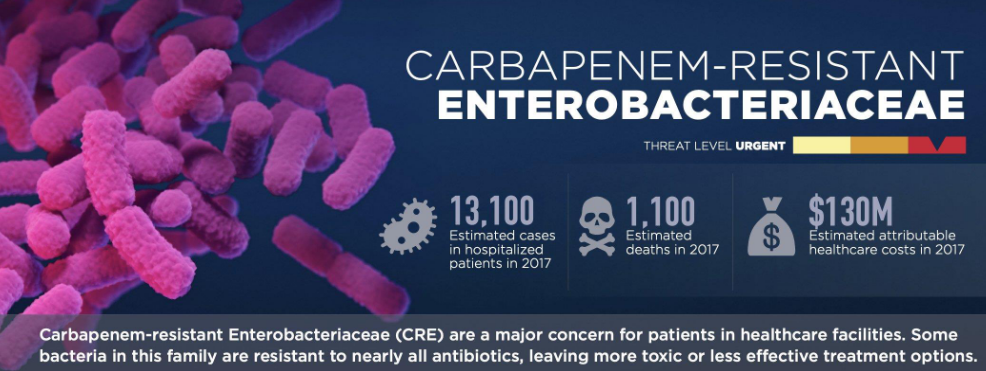
Figure 10.11: CRE Infographic
These include Klebsiella and E. coli - normal bacteria of the human gut that can become resistant to carbapenem. Consequently, these bacteria can cause infections including pneumonia, bloodstream infections, UTIs, wound infections, and even meningitis. These infections also take place in hospitals for the most part.
Types of CRE include Klebsiella pneumoniae carbapenemase (i.e., KPC) and New Delhi Metallo-beta-lacatamase (i.e., NDM): these are enzymes that degrade carbapenem and make it ineffective.
Carbapenems are a type of \(\beta\)-lactam antibiotic - a “drug of last resort.” Up to 50% of patients who become infected will die from CREs.
10.6.3 Drug resistant *Neisseria gonorrhoeae**
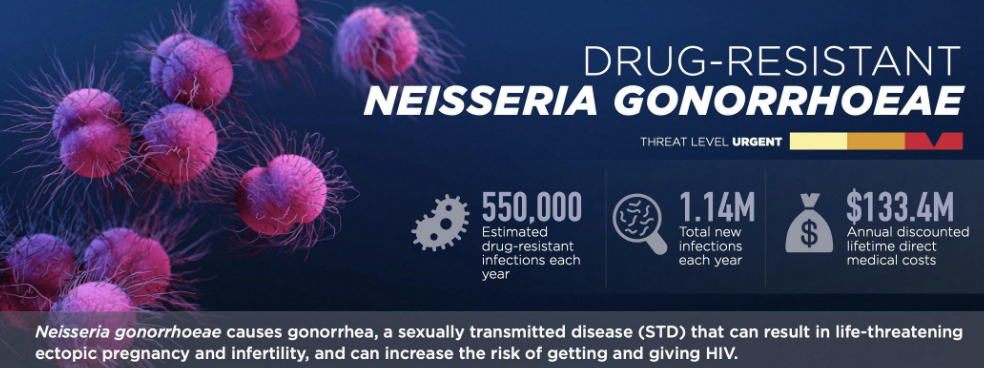
Figure 10.12: N. gonorrhoeae Infographic
These bacteria are the cause of sexually transmitted infections (STIs) gonorrhea.
These bacteria are also obligate human pathogens that are highly evolved to persist in the human population.
In males, there is a urethrla discharge of yellow, creamy pus, and painful, burning urination.
In females, there is vaginal discharge from 7 to 21 days after the initial infection period, but gonorrhea is often asymptomatic and if untreated, can lead to fallopian tube infections. Because of this, gonnorhea is also considered to be a major cause of infertilit yand ectopic pregnnancies.
In some cases, disseminated gonococcal infections can involve the movement of joints, the heart; however, this rarely causes death.
10.6.3.1 Current status of *N. gonorrhoeae infections
N. gonorrhoeae has slowly developed resistance to every antibiotic drug prescribed to treat it. Current treatment guidelines in the US are dual therapy with injectable ceftriaxone and oral azithromycin.
Dual therapy is needed to address the problem of a potential emergence “gonococcal cephalosporin resistance” - the so-called “ticking time bomb.”
10.6.4 Methicilin-resistant Staphylococcus aureus (MRSA)
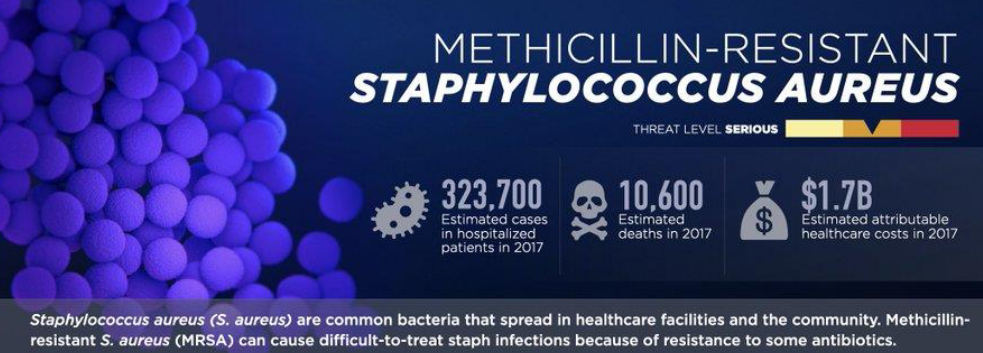
Figure 10.13: Methicilin-Resistant S. aureus
S. auereus is a normal inhabitant of the upper respiratory tract, the skin, the intestines, and the vagina.
However, they can be harboed by asymptomatic carriers or active carriers - they can also be spread by hands, inanimate objects, or expelled via the respiratory tract or through blood.
MRSA can cause disease in almost every organ and tissue - the immunocompromised are the most at risk groups.
10.6.5 Drug-resistant non-typhoidal Salmonella
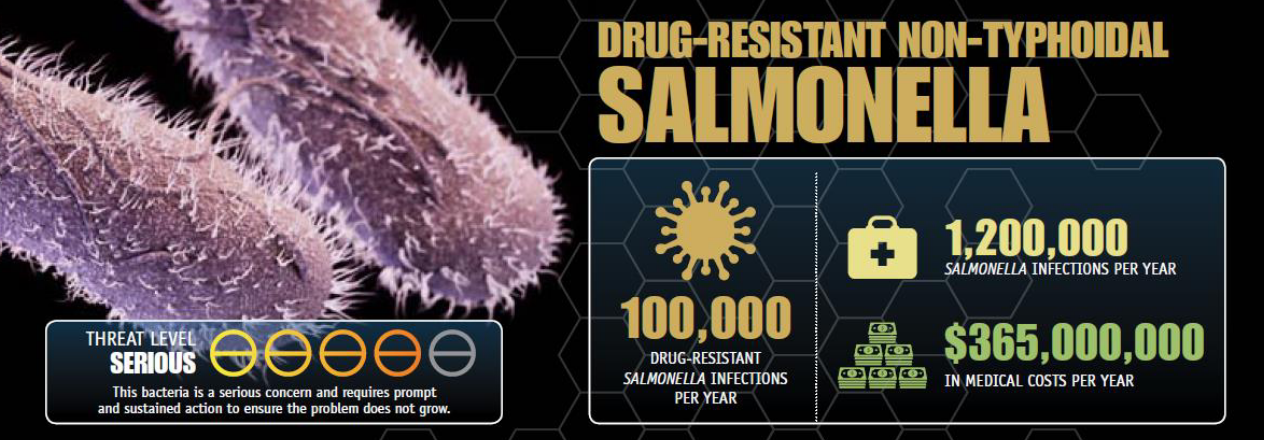
Figure 10.14: Drug-Resistant, Non-Typhoidal Salmonella
These bacteria are transmitted to humans via foods such as beef, poultry, eggs, and water. Disease from this bacteria are a result of enterotoxin and cytotoxin production from the bacteria in the intestinal mucosa.
Symptoms include abdominal pain, cramps, diarrhea, nausea, vomiting, and fever that lasts about 2 - 5 days.
10.6.6 Drug-resistant Salmonella serotype typhi

Figure 10.15: Typhus-Causing Salmonella
This bacteria is acquired by ingesting food or water that have been contaminated by the feces of infected humans or person-to-person contact.
The incubation period of this bacteria is between 10 - 14 days, and symptoms include feve,r headache, abdominal pain, anorexia, and malaise.
10.6.7 Typhus
The bacteria that cause typhus spread from the small intestine to the lymph tissue, the blood, the liver, and the gallbladder - typhus is also associated with pre-term labor and abortion.
An infected person can shed bacteria for up to three months - in asymptomatic carriers (e.g., Typhoid Mary), bacteria grow in the gallbaldder and reach the intestines via the bile duct.
Antibiotic therapy, vaccines, and purifying drinking water are all part of treatment, prevention, and control methods for dealing with Typhus.