Chapter 3 Endocrine System (part I)
The endocrine system is a collection of ductless glands that secrete hormones. These glands are not only specialized (i.e., they each serve a unique purpose), but are also essential for homeostasis and are found in the hypothalamus adipose tissue (e.g., leptin is a satiety hormone), and the gastrointestinal tract (e.g., the glucose-inhibiting-peptide and grehlin - the “hunger” hormone).
3.1 Hormones
3.1.1 Classifying hormones
Hormones can be classified into three main types:
Peptide hormones are made from amino acids; these include insulin, ADH (i.e., vasopressin), and TRH (made from glutamine, histamine, and proline).
Large peptide hormones (e.g., glycoproteins; larger than 100 kD) are bound to one or more carbohydrate groups.
Amine hormones are derived from amine compounds.
Steroid hormones are hormones that have been derived from cholesterol: these include testerone, estrogen, and progesterone.
3.1.2 Mechanisms of hormone action
The effects of different hormones are mediated by specific hormone receptors in the cell; the location of the receptor depends on the nature of the hormone itself.
As a general rule of thumb, hydrophobic hormones (e.g., steroid hormones) have intracellular receptors (nuclear or cytoplasmic), whereas receptors for hydrophilic hormones are on the cell surface.
Furthermore, there are three different hormone receptors on the cell surface:
G-protein linked receptors serve to activate a second chemical messager pathway.
Ion-channel linked receptors are mainly for neuropeptide hormones.
Enzyme-linked receptors are mostly for protein kinases (e.g., the insulin receptor is a tyrosine kinase receptor).
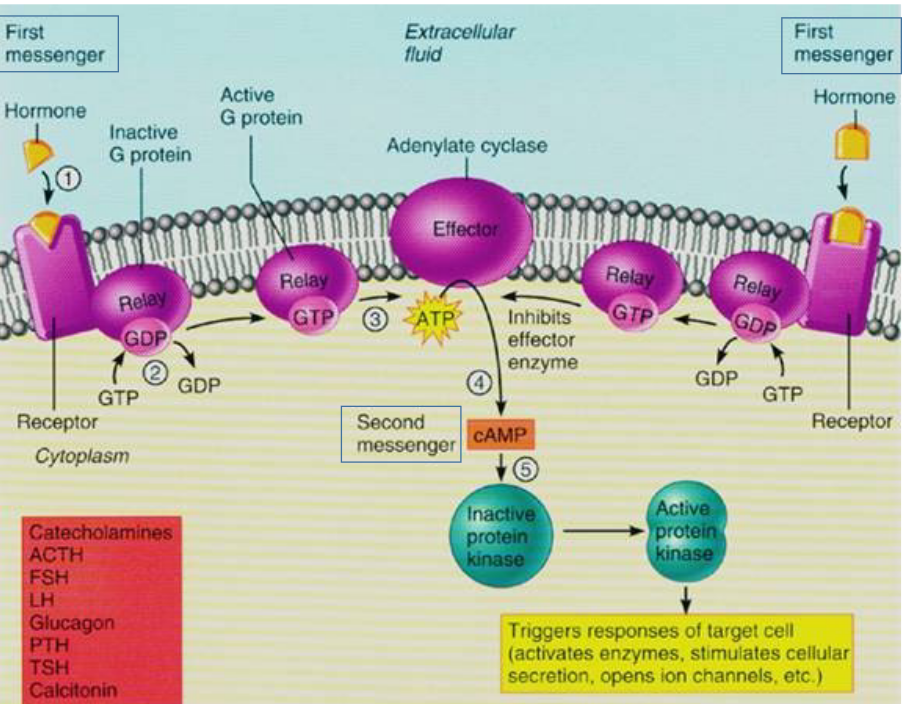
Figure 3.1: The G-protein Receptor in Action
3.2 Regulating the Endocrine System
Hormone secretions are not only tailored to the internal and the external environment (of the person), but they can also be regulated via the three feedback mechanisms of homeostasis described in the previous chapter!
Hormone secretions are also responsible for the maintenance of the circadian rhythm and neuroendocrine reflexes (e.g., secreting oxytocin to prepare the mother for labor).
Tissue sensitivity is influenced by tissue receptors and transcription co-factors.
Hormone binding to plasma proteins can also cause activation in organs (e.g., the liver and the kidneys).
3.2.1 Endocrine System Disorders
Most endocrine disorders are from the hyposecretion or hypersecretion of a hormone.
Hyposecretion (i.e., inadequate secretions) of a hormone may be due to a genetic or dietary deficiency and may be the primary or secondary cause of a disease. In most cases, hormone replacement therapy is a suitable treatment.
Hypersecretion (i.e., oversecretion) of a hormone may be due to tumors of the endocrine gland and immunological factors.
Furthermore, a lack of tissue response may also cause endocrine dysfunction (e.g., type II diabetes and testicular feminization syndrome).
3.3 Central Endocrine Glands
There are four central glands - they are the:
- Hypothalamus
- Anterior pituitary gland
- Posterior pituitary gland
- Pineal gland
3.3.1 Hypothalamus
This forms the lower lateral walls and the floor of the third ventricle above the pituitary gland. Furthermore, the hypothalamus is also connected to structures in the limbic system and in the brainstem.
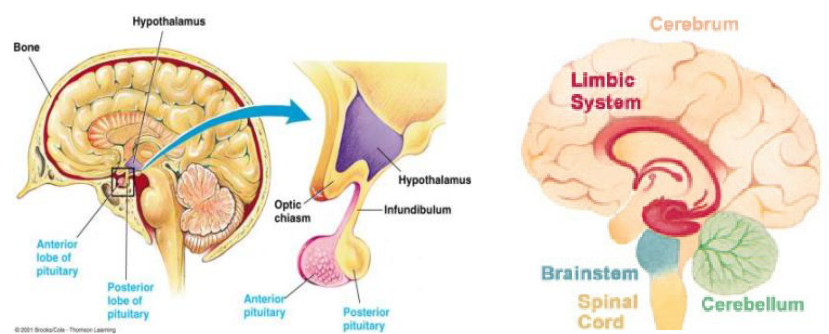
Figure 3.2: Structure of the Hypothalamus
The hypothalamus is also an integrating center for many homeostatic functions - it releases hormones that regulates the secretion of the anterior pituitary.
3.3.2 Pituitary gland
This gland is attached to the hypothalamus via the infundibulum. It is divided into two portions: the anterior lobe and the posterior lobe.
The anterior lobe is made up of glandular tissue - adrenohypophysis happens here.
The posterior lobe is made up of neural tissue - neurohypophysis happens here.
3.3.2.1 Secretions from the anterior pituitary gland
The hormones made here are:
Adrenocorticotropic hormones (i.e., ACTH or corticotropin)
This stimulates the adrenal cortex to make corticosteroids
Thyroid-stimulating hormone (i.e., TSH)
This stimulates the thyroid to make thyroxine.
Lutenizing hormone (i.e., LH)
This is needed for ovulation and for the formation of the corpus luteum. This causes the testes to make testosterone.
Follicle-stimulating hormone (i.e., FSH)
This is required for the development of ovarian follicles in females - this hormone causes sperm development in males.
Prolactin
This induces the labular-aveolar growth of the mammary gland and induces lactogenesis (i.e., milk production).
Growth hormone
This promotes the growth of tissues.
All hypothalamic hormones are transported to the anterior pituitary via the hypothalamic-hypophyseal portal system: a system of blood vessels connecting capillaries in the hypothalamus with capillaries in the anterior pituitary gland.
3.3.2.2 Secretions of the posterior pituitary gland
The hormones made here are:
Thyrotropin-releasing hormonea (i.e., TRH)
This releases TSH.
Corticotropin-releasing hormone (i.e., CRH)
This stimulates the release of ACTH.
Gonadotropin-releasing hormone (i.e., GnRH)
This stimulates the secretion of FSH and LH.
Growth hormone-releasing hormone (i.e., GHRH)
This stimulates the release of the growth hormone.
Growth hormone-inhibiting hormone (i.e., GHIH or Somatostatin)
This inhibits the release of the growth hormone.
Prolactin-releasing hormone (i.e., PRH)
This inhibits the secretion of prolactin.
Prolactin-inhibiting hormone (i.e., PIH)
This stimulates the release of dopamine.
Negative feedback from the target gland can also act on the anterior pituitary gland and the hypothalamus to stop the secretion of stimualting and releasing hormones.
3.3.3 Hypothalamus-pituitary adrenal / gonadal axis
This axis is regulated in the brain. When an individual is stressed, there is a higher amount of CRH and ACTH released (and hence, a higher amount of corticosteroids too). Stress also affects the timing of menstruation too.
The dormitory effect refers to a delay in the menstrual cycle - this is believed to be caused by pheromones, but this is still up for debate.
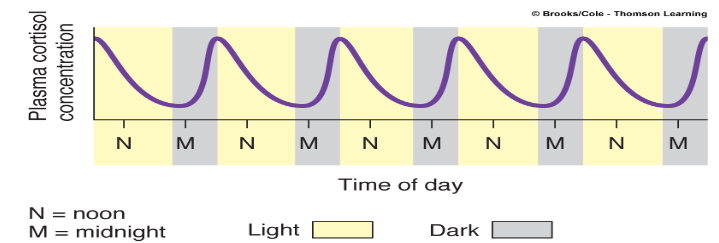
Figure 3.3: Circadian Rhythms
Circadian rhythms refer to the pattern of cortisol secretions - it is highest during sleep and lowest during wakefulness.
3.3.4 Growth hormone
This stimulates the growth of muscle, bone, and cartilage.
Growth hormone also increases protein synthesis, maintains the level of blood glucose (via decreasing glucose uptake and enhancing glycogenesis), and mobilizes fat via lipolysis and fatty acid oxidation in adipocytes.
The growth hormone directly exhibits its effects via the GH receptor and indirectly exhibits its effects via the IGF-I from the liver and the other tissues.
3.4 Structure of the Bone
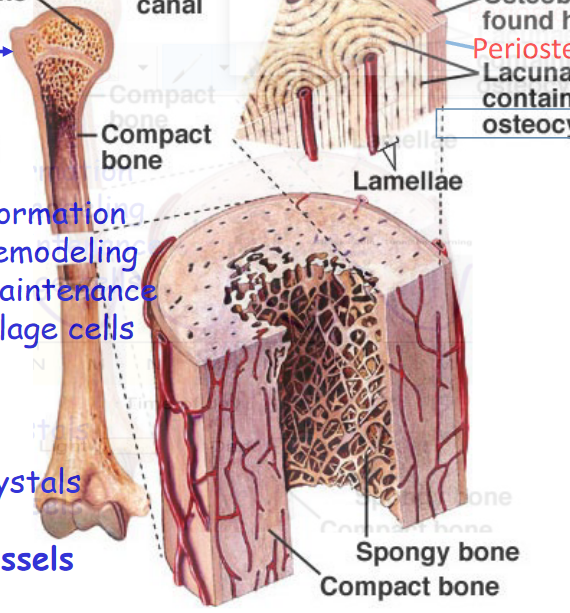
Figure 3.4: Structure of the Bone
There are four kinds of bone cells:
Osteoclasts
These are involved in bone remodeling
Osteoblasts
These are invovled in bone formation
Osteocytes
These are responsible for bone maintenance
Chondrocytes
These are responsible for producing cartilage
The matrix of the bone is made up of calcium phosphate (i.e., Ca3(PO4)2) crystals, collagen fibers, and also nerve and blood vessels.
The growth hormone stimulates the lengthening of the bone via enhancing osteoclast and chondrocyte activity.
3.4.1 How do bones widen?
Osteoblasts first deposit a matrix of calcium phosphate crystals and osteoclasts carry out bone resorption on the inner side of the bone.
IGF-1 also stimulates the activity of osteoclasts and osteoblasts.
3.4.2 Growth hormone secretions
Secretions of growth hormones are highest during sleep and are lowest during periods of wakefulness (as mentioned previously).
Exercise and a diet high in amino acids (i.e., a high-protein diet) and low in glucose increase the secretion of the growth hormone.
A deficiency in the growth hormone leads to a condition called dwarfism. Gigantism and acromegaly are conditions that result from excessive growth hormone secretion.
3.4.2.1 Other hormones for proper bone growth
The effect of the growth hormone (on the bones) can only be felt when there are sufficient amounts of thyroid hormones present in the person.
Androgens play an important role in pre-pubescent growth spurts and protein synthesis. Not only are androgens responsible for muscle development in men, but they are also responsible for the ossification of the epiphyseal plate.
Estrogen also has a similar effect to androgens on the bone.
3.5 Posterior Pituitary Hormones
The posterior pituitary gland - like mentioned previously - secretes vasopressin and oxytoxin.
3.5.1 Vasopressin
Vasopressin (i.e., ADH) is a hormone that stimulates the insertion of water channels into the membranes of kidney tubules. High concentrations of ADH can cause smooth muscle contractions.
The role of ADH is to maintain blood osmolarity and volume - the major stimulus for ADH release is an increase in the osmolarity (i.e., a hypertonic blood plasma) of the blood plasma (which is detected by osmoreceptors).
The decrease in blood flow and pressure (detected by the left atrial receptor) also stimulates the secretion of ADH.
3.5.2 Oxytocin
Oxytocin stimulates the contraction of the uterus during labor - labor is initiated when oxytocin receptor concentrations reach a threshold.
Oxytocin also sitmulates the contraction of the mammary aveoli to facilitate milk-ejaculation.
Interestingly, oxytocin has also been suggested to be involved in mother-infant bonding (i.e., oxytocin infusion facilitates pair bonding; oxytocin antagonists prevent pair bonding) and positive emotions in humans.
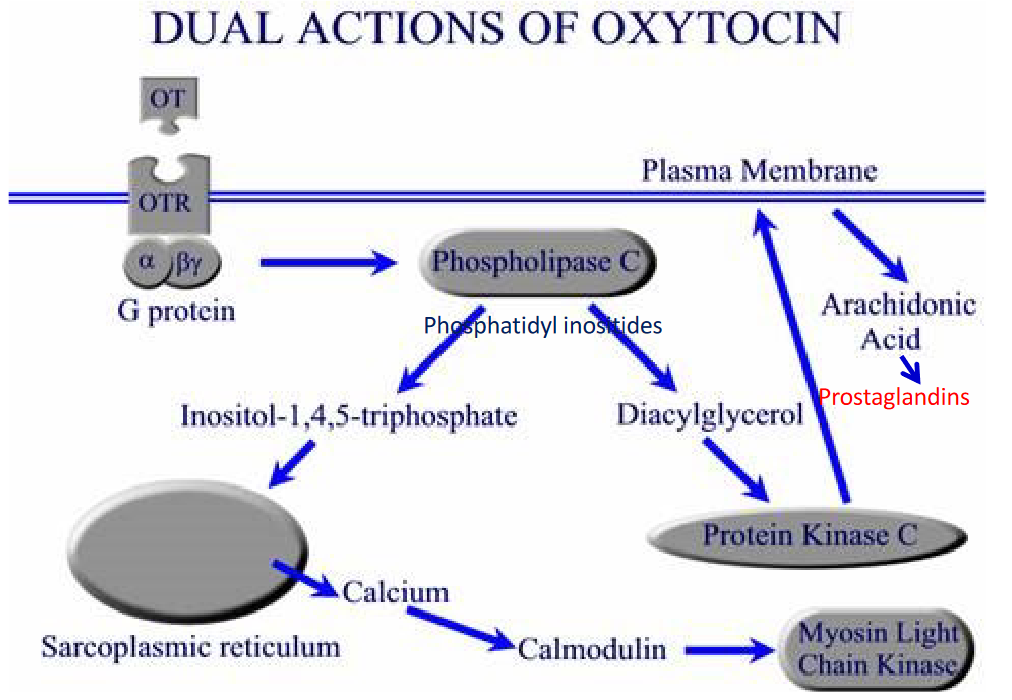
Figure 3.5: Oxytocin Receptor Actions
The oxytocin receptor is a G-protein linked receptor.
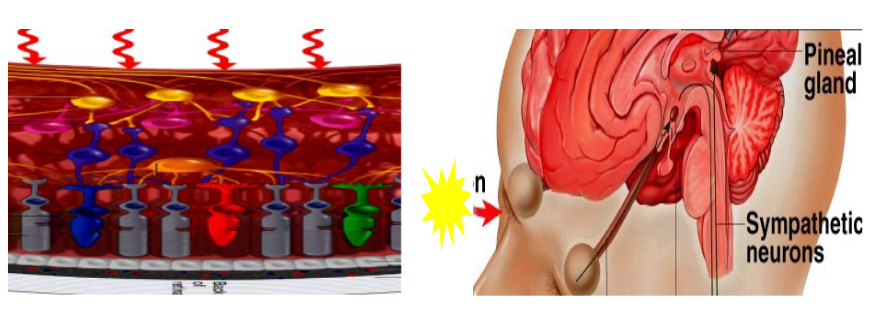
3.6 Pineal Gland
This is a tiny, cone-shaped structure in the center of the brain:
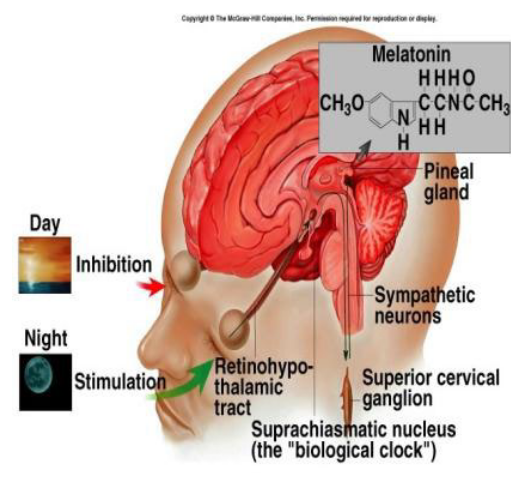
Figure 3.6: The Pineal Gland
The gland secretes melatonin after the middle night (i.e., after 2 AM). Secretions are controlled by inputs from the suprachiasmatic nuclei (i.e., SCN) - these are the so-called pacemaker of the circadian rhythms.